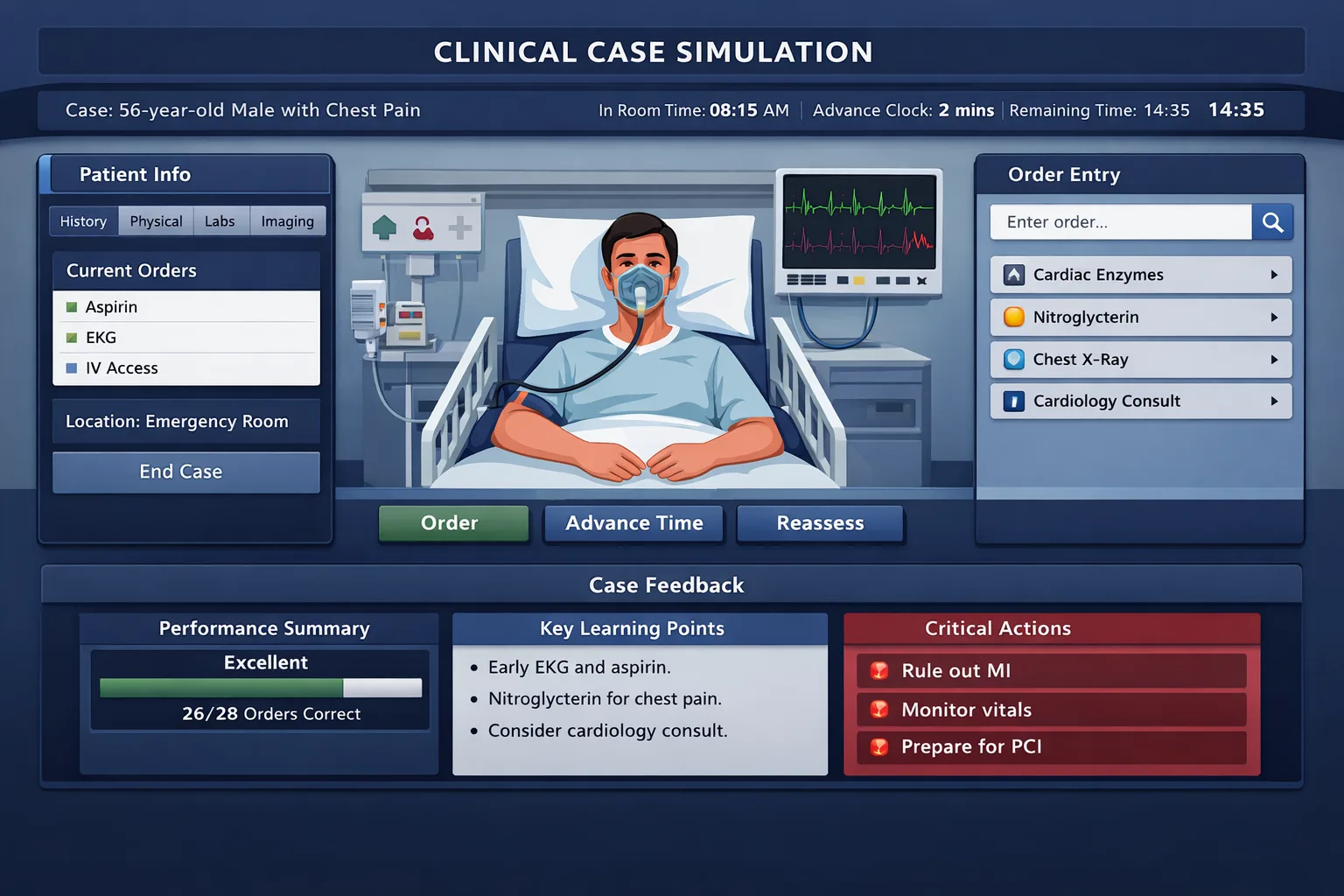
Step 3 CCS case mistakes usually come from a weak system, not a weak fund of knowledge. This guide shows how to prevent the errors that cost points: delayed stabilization, incomplete monitoring, poor simulated-time control, missed disposition, and forgotten preventive care. The CCS portion of USMLE Step 3 tests whether a physician can manage an undifferentiated patient in a simulated clinical environment. It is not a simple diagnosis game. The case responds to your orders, location decisions, monitoring, timing, and counseling. That is why many residents who are clinically capable still lose points. They know the diagnosis, but they do not translate that knowledge into a complete sequence of actions inside the software. The most common pattern is premature narrowing. A learner sees crushing chest pain and thinks only of myocardial infarction. They order an ECG and troponin, then advance time. The case may require cardiac monitoring, oxygen when indicated, IV access, aspirin when appropriate, pain control, contraindication checks, cardiology consultation, admission level, and follow-up testing. The diagnosis was not the problem. The management frame was incomplete. Another recurring problem is treating CCS like a multiple-choice question. On MCQs, the correct answer may be a single best test or treatment. In CCS, a safe plan is a bundle. A sick patient needs immediate stabilization before a full diagnostic workup. A stable outpatient needs targeted history, appropriate examination, diagnostic confirmation, risk modification, screening, and follow-up. A hospitalized patient needs reassessment and monitoring before simulated time is advanced. The exam rewards the behavior of a general physician who recognizes acuity and manages risk. USMLE describes CCS as a dynamic simulation of patient-care situations. The patient can improve, worsen, or remain unchanged as simulated time passes. Therefore, every time you advance the clock, you are making a clinical bet that the patient is safe enough to wait. This is the central mental model. The clock is not a navigation button. It is a treatment decision. Most poor CCS performances share five defects: no initial triage, missing safety orders, incomplete targeted workup, unsafe time advancement, and weak closure. These are fixable. The goal is to build a reproducible sequence that applies across emergency department, inpatient, intensive care, office, and home settings. Ordering a diagnostic panel before stabilizing an unstable patient misses the logic of emergency care. The patient may deteriorate if monitoring, treatment, or reassessment has not been placed. Triage, stabilize, diagnose, treat, monitor, reassess, disposition, and counsel. A strong CCS approach begins with one question: “Can this patient safely stay where they are while I think?” If not, move them or stabilize them. A hypotensive patient in the office belongs in the emergency department. A patient with respiratory failure belongs in the emergency department or ICU. A patient with altered mental status, shock, active bleeding, sepsis, or suspected stroke should not be managed as a routine outpatient. Location errors are especially costly because every later order is built on the wrong care setting. Once the setting is appropriate, the next question is: “What harm can occur in the next few minutes?” That question leads to pulse oximetry, cardiac monitoring, IV access, oxygen when hypoxemic, fluids when shock is likely, glucose testing in altered mental status, pregnancy testing before teratogenic imaging or medications, and cultures before antibiotics when sepsis is likely and collection will not delay care. These orders are not “extras.” They are expressions of clinical safety. MDSteps teaches this as a management habit rather than a memorized script. Within the Step 3 preparation pathway, CCS practice should train the same sequence repeatedly until the interface no longer consumes attention. When the mechanics become automatic, working memory is freed for diagnosis, contraindications, and time-sensitive treatments. The first major CCS error is failing to decide whether the patient is in the right place. Examinees often begin typing orders before answering the most important management question: does this presentation require escalation? CCS cases may begin in an office, emergency department, inpatient unit, intensive care unit, or home context. A patient with red flags must be moved to a setting that can support urgent evaluation and treatment. Common red flags include hypotension, severe hypoxemia, altered mental status, chest pain with instability, acute neurologic deficit, severe abdominal pain with peritoneal findings, anaphylaxis, suicidal intent, active GI bleeding, postpartum hemorrhage, diabetic ketoacidosis, sepsis physiology, status asthmaticus, and suspected ectopic pregnancy. A stable outpatient with chronic hypertension does not need an ICU. A febrile, hypotensive patient with confusion should not stay in clinic while outpatient labs are ordered. On CCS, triage is not just a clinical principle. It controls what orders make sense. Cardiac monitoring belongs in an acute setting. Serial vital signs matter more when physiology is unstable. Consults, admission, procedures, and timed reassessment depend on location. If the patient is placed incorrectly, your plan may look disorganized even if individual orders are reasonable. A practical rule is to decide location before diagnosis when the patient looks sick. You do not need a final diagnosis to move a patient with shock, severe respiratory distress, or new focal neurologic deficit. You need a safe environment. In board-style logic, management follows the sequence of stabilization, targeted diagnosis, definitive therapy, and disposition. This sequence is tested repeatedly across Step 2 CK and Step 3, but CCS makes the sequence active. Do not confuse “complete evaluation” with “safe evaluation.” In an unstable patient, a focused physical examination is often better than a lengthy one. A patient in shock does not need a comprehensive skin, neurologic, and musculoskeletal examination before resuscitation begins. A stable patient with chronic fatigue may benefit from a more complete exam and slower diagnostic strategy. The error is using the same exam template for every case. NBME-style traps often punish the wrong tempo. If a patient presents with sudden severe chest pain radiating to the back and pulse deficit, the dangerous diagnosis is aortic dissection. Anticoagulation before considering dissection can be harmful. If a pregnant patient has abdominal pain and syncope, ectopic pregnancy must be considered early. If a patient has fever, neck stiffness, and altered mental status, delayed empiric therapy can be dangerous. CCS rewards clinicians who recognize dangerous possibilities while still ordering reasonable confirming tests. Many candidates lose time because they attempt to perfect the differential before acting. That is backwards in emergencies. You can stabilize without knowing every detail. You can start oxygen for hypoxemia, establish IV access, obtain glucose, place the patient on a monitor, and order urgent diagnostics while the differential remains broad. The patient does not need your final answer. The patient needs a safe next step. The best prevention strategy is a two-word checkpoint: “location first.” Before every case, name the setting. Then name the acuity. If the patient is unstable, escalate. If stable, proceed deliberately. This simple habit prevents many downstream mistakes because it forces the exam taker to think like a supervising physician rather than a test taker collecting facts. The second common error is diagnostic enthusiasm before stabilization. CCS cases are built to evaluate patient management, not just pattern recognition. A long list of labs cannot substitute for immediate actions that reduce risk. For example, in suspected sepsis, cultures and lactate are important, but fluid resuscitation, early antibiotics, source evaluation, and ongoing reassessment are the management frame. In acute coronary syndrome, ECG and troponin matter, but so do monitoring, antiplatelet therapy when appropriate, symptom control, contraindication review, and disposition. Stabilization does not mean placing every possible order. It means addressing the physiologic threats suggested by the presentation. Airway compromise requires airway management and urgent help. Hypoxemia requires oxygen and respiratory support. Shock requires IV access, fluids when appropriate, vasopressors in selected cases, and monitoring. Hypoglycemia requires dextrose. Seizures require acute antiseizure treatment. Anaphylaxis requires epinephrine. These are high-yield CCS actions because they show that you can protect the patient while diagnostic work proceeds. One danger is using “shotgun orders” without clinical logic. A broad order set can help memory, but it can also lead to irrelevant testing, delayed priorities, and missed contraindications. The safer approach is a tiered system: universal safety orders for unstable patients, syndrome-specific diagnostic orders, definitive treatment, and monitoring. This keeps speed without sacrificing reasoning. Testing should be targeted to dangerous and likely diagnoses. In abdominal pain, pregnancy test is essential in reproductive-age patients. In syncope, ECG is often a core order because arrhythmia can be lethal. In suspected stroke, noncontrast head CT and glucose are time-sensitive. In suspected pulmonary embolism, oxygenation, hemodynamic status, risk stratification, and imaging selection all matter. In possible meningitis, blood cultures and empiric antimicrobials should not be delayed by low-yield testing when the patient is ill. CCS also tests therapeutic timing. An unstable patient often needs treatment before all confirmatory results return. A stable patient may need confirmation before definitive therapy. This distinction is essential. Treat suspected septic shock early. Do not delay epinephrine in anaphylaxis. Do not delay glucose in severe hypoglycemia. Conversely, do not give thrombolytics for stroke without appropriate imaging and eligibility review. Do not anticoagulate a patient when the stem suggests aortic dissection until that threat is addressed. A useful phrase is “diagnose while treating.” This keeps your orders parallel. You can order CBC, CMP, cultures, imaging, ECG, urinalysis, pregnancy test, and other indicated tests while also ordering fluids, oxygen, analgesia, antiemetics, antibiotics, bronchodilators, or other appropriate therapies. CCS rewards concurrent management when the case requires it. Practice should emphasize sequence more than memorization. After every case, ask: did I protect airway, breathing, circulation, neurologic status, pregnancy safety, and patient safety before waiting? Did I order monitoring before moving time? Did my treatment match the most dangerous likely diagnosis? These questions turn errors into a reusable checklist. Move beyond knowing the diagnosis and practice what to do next as the patient changes. Unsafe time advancement is one of the most damaging CCS habits. In the software, advancing time may feel like clicking “next.” Clinically, it means you are allowing the patient to live with your current orders for minutes, hours, days, or months. If you advance before monitoring is in place, you may miss deterioration. If you advance before treatment is started, you may allow a reversible condition to worsen. If you advance too slowly in a stable case, you may waste real time and fail to reach closure. The key is to pair time with physiology. A critically ill patient should be reassessed quickly after initial orders. A stable outpatient may be reassessed after days or weeks depending on the problem. A hospitalized patient with pneumonia may need several hours of observation before improvement is expected. A patient starting a chronic medication may need outpatient follow-up in weeks. CCS performance improves when time movement reflects clinical tempo. Monitoring should be specific. Cardiac monitor is appropriate for arrhythmia risk, chest pain, syncope with concerning features, electrolyte disturbance, overdose, and unstable physiology. Pulse oximetry is appropriate for respiratory complaints, sedation risk, severe infection, and hypoxemia. Serial vital signs are important in acute illness. Intake and output may matter in kidney injury, heart failure, sepsis, and DKA. Fingerstick glucose matters in diabetes, altered mental status, and insulin therapy. Fetal monitoring is relevant in selected obstetric scenarios. Do not order monitoring as decoration. Use it to guide reassessment. If you give fluids, check blood pressure, heart rate, urine output, respiratory status, and signs of overload. If you give insulin for DKA, monitor glucose, electrolytes, anion gap, and potassium. If you treat asthma, reassess work of breathing, oxygen saturation, and peak flow when appropriate. If you treat pain, reassess pain and adverse effects. A monitor without reassessment is only half a management decision. A common trap is advancing to “next available result” when no stabilizing orders have been placed. Another is advancing several hours after ordering antibiotics without checking whether the patient improves. A third is advancing days after initiating a medication that needs safety monitoring. In real clinical practice, these errors are caught by nurses, teams, and electronic alerts. In CCS, the examinee must create the safety net. Timing also matters in preventive and outpatient cases. A patient with newly diagnosed hypertension should not be sent to the ICU, but the case still needs follow-up, lifestyle counseling, medication selection when indicated, and monitoring for adverse effects. A patient with depression needs safety assessment, treatment plan, and follow-up. A patient with diabetes needs glycemic monitoring, cardiovascular risk assessment, kidney screening, eye care, foot care, and medication safety. Time advancement should show continuity, not abandonment. The most efficient habit is a “before I wait” pause. Before any time jump, ask: what could kill or seriously harm this patient while I wait? What measurement will tell me whether the patient is improving? What result do I need before the next decision? If you cannot answer those questions, do not advance yet. Order the missing monitor, treatment, consult, or reassessment first. This is where timed practice matters. The MDSteps live vitals CCS cases are designed to make learners practice timed orders with real physiology. That format is useful because it teaches the relationship between a management decision and the patient’s response, which is the skill CCS is trying to sample. Many candidates handle acute diagnosis and treatment but forget the final layer of care: contraindications, counseling, prevention, and patient education. CCS is not only about saving the patient in the first five minutes. It also evaluates whether the physician closes the loop. A patient discharged after myocardial infarction needs risk-factor modification, medication education, follow-up, and safety instructions. A patient treated for PID needs partner management and counseling. A patient with alcohol withdrawal needs treatment, relapse planning, and appropriate support. A patient with diabetes needs education and monitoring, not just a glucose-lowering order. Contraindications are high-yield because they distinguish reflexive ordering from physician judgment. Before anticoagulation, consider active bleeding, intracranial hemorrhage risk, recent surgery, severe thrombocytopenia, pregnancy context, and suspected dissection. Before CT with contrast, consider kidney function and allergy when relevant. Before teratogenic medications or imaging, consider pregnancy. Before beta-blockers, consider severe bradycardia, hypotension, and acute decompensated heart failure. Before NSAIDs, consider kidney disease, GI bleeding risk, and pregnancy stage. The point is not to avoid treatment. The point is to treat safely. Counseling orders can feel less urgent, but they are often part of complete care. Smoking cessation, alcohol counseling, safe sex counseling, diet and exercise, medication adherence, return precautions, fall prevention, intimate partner violence resources, and immunization counseling may be appropriate depending on the case. In CCS, these are not substitutes for lifesaving care. They come after stabilization and management, usually near the end of the case or during outpatient follow-up. Preventive care is especially important in office cases. Examinees often over-order acute tests and under-order screening. A middle-aged patient with a chronic disease visit may need cancer screening, vaccination review, cardiovascular risk assessment, depression screening, and lifestyle counseling. A pregnant patient needs prenatal care logic. An older adult may need fall risk assessment, medication review, and immunizations. Preventive care should be guided by age, sex, pregnancy status, risk factors, and current recommendations. Do not let counseling crowd out emergency management. The sequence matters. In a patient with septic shock, tobacco counseling can wait. In a stable outpatient with COPD, smoking cessation may be central. In a patient with suspected stroke, imaging and reperfusion eligibility matter before diet counseling. CCS rewards proportionality. The right order at the wrong time may still reflect poor clinical judgment. Another frequent error is forgetting to discontinue harmful or unnecessary orders. If the diagnosis changes, the plan should change. If a patient was initially NPO and later stable for discharge, diet and outpatient instructions should match the new state. If empiric antibiotics are narrowed after culture results, the case should reflect that. If IV fluids become risky in heart failure, reassess and adjust. Step 3 often tests adaptive management rather than static protocols. A strong closure checklist includes diagnosis, definitive treatment, monitoring plan, counseling, prevention, disposition, and follow-up. This is the moment to add education that fits the patient. For example, after treating DKA, address insulin adherence, sick-day rules, glucose monitoring, and follow-up. After treating asthma exacerbation, address inhaler technique, triggers, controller therapy when indicated, and return precautions. After treating a sexually transmitted infection, address partner notification, abstinence until treatment completion, and screening for coinfections when appropriate. Think of counseling and prevention as the final proof that you understood the case. Stabilization shows safety. Diagnostics show reasoning. Treatment shows knowledge. Counseling, prevention, and follow-up show physician ownership. CCS errors occur at both extremes. Some examinees under-order because they are afraid of doing too much. Others over-order because they hope a broad panel will collect points. Neither approach is ideal. A safe CCS plan is comprehensive where the patient is at risk and restrained where testing adds little value. The exam expects generalist judgment, not maximal resource use. Under-ordering often comes from relying on the diagnosis alone. A learner recognizes DKA and orders insulin but forgets potassium, fluids, glucose monitoring, electrolytes, anion gap tracking, infection search, and disposition. Another recognizes pneumonia but forgets oxygenation, blood cultures when severe, antibiotics, admission criteria, and reassessment. Another recognizes ectopic pregnancy but forgets pregnancy test, ultrasound, hemodynamic assessment, Rh status, OB/GYN consultation, and surgical readiness if unstable. Over-ordering usually comes from anxiety. The candidate orders CT scans, autoimmune panels, tumor markers, broad toxicology, extensive infectious workups, and multiple consults without a clear indication. This can waste time and may introduce harmful choices. For example, unnecessary invasive testing can be inappropriate in a stable patient with a straightforward outpatient diagnosis. Unnecessary imaging may be unsafe in pregnancy. Excessive broad-spectrum antibiotics without a reasonable infectious syndrome may not reflect good stewardship. The solution is to keep the case thread visible. The thread includes the chief problem, acuity, dangerous diagnoses, likely diagnosis, immediate management, expected response, and next decision. Every order should attach to one of those elements. If an order does not stabilize, diagnose, treat, monitor, prevent harm, determine disposition, or educate the patient, it may not belong. Before placing a questionable order, ask whether it does one of the following: Consultation is another area where candidates drift. Consults are appropriate when a patient needs procedural expertise, specialty admission, operative management, complex decision-making, or urgent intervention. They should not replace basic physician action. In suspected STEMI, cardiology may be needed, but the initial physician still orders ECG, monitoring, aspirin when appropriate, and stabilization. In ectopic pregnancy with instability, OB/GYN is urgent, but resuscitation cannot wait. In suicidal ideation, psychiatry matters, but safety precautions and medical stabilization are still your responsibility. Order sequencing should also respect diagnostic uncertainty. For example, chest pain may be ACS, dissection, pulmonary embolism, pneumothorax, GERD, or anxiety. The initial plan should identify lethal diagnoses and not commit prematurely to one. Severe headache may be subarachnoid hemorrhage, meningitis, migraine, hypertensive emergency, or mass lesion. A focused neurologic exam, vital signs, imaging choice, and infection assessment keep the thread intact. A useful after-action review is to write missed orders into categories, not random lists. Category labels might include stabilization, monitoring, diagnostic confirmation, contraindication, treatment, consult, disposition, prevention, and follow-up. If the same category appears repeatedly, that is the habit to fix. A student who repeatedly misses monitoring needs a “before time advance” checkpoint. A student who misses counseling needs a case-closure checklist. A student who orders too broadly needs the seven-order filter. The highest-yield practice is not doing hundreds of cases passively. It is reviewing why each missed order mattered. The MDSteps Adaptive QBank, automatic study plan generator, readiness dashboard, AI tutor, and flashcard decks generated from misses can help connect CCS-style mistakes to broader Step 3 knowledge gaps. The goal is not to memorize every case. The goal is to stop repeating the same management error in new clothing. A repeatable workflow protects you from exam-day variability. The details change by case, but the skeleton remains stable: read setting and vitals, triage, perform the appropriate examination, stabilize, diagnose, treat, monitor, reassess, decide disposition, and close with counseling and follow-up. This structure prevents cognitive overload because you no longer decide from scratch what “doing a case” means. Start with the opening screen. Identify age, sex, location, chief concern, vital signs, pregnancy possibility, and obvious red flags. Do not skip the location. An office case and an emergency department case have different tempos. Next, choose the exam. If the patient is unstable, perform a focused exam relevant to immediate threats. If stable, a fuller exam is reasonable. Avoid reflexive comprehensive exams in crashing patients. Then place stabilization orders when indicated. These may include IV access, cardiac monitor, pulse oximetry, oxygen for hypoxemia, fluids for shock, analgesia, antiemetics, glucose testing, airway support, or other immediate therapies. Next, order syndrome-specific diagnostics. Keep dangerous diagnoses in view. For chest pain, consider ECG and cardiac markers, but also dissection, PE, pneumothorax, and GI causes when the presentation suggests them. For abdominal pain, consider pregnancy, surgical abdomen, urinary causes, vascular disease, and infection. Treatment follows probability and danger. Some treatments are empiric because delay is risky. Others require confirmation. This is where Step 3 management logic matters. Stabilize first. Test when results change management. Treat immediately when delay harms the patient. Avoid harmful treatment when a dangerous contraindication is plausible. Reassess after therapy. Disposition is a common late-case failure. A patient who improves after ED treatment may still need admission if the underlying risk remains high. A patient with uncomplicated outpatient disease may need follow-up rather than hospitalization. A patient with psychiatric danger may need safety measures and appropriate placement. A patient with an operative abdomen needs surgical consultation and likely admission. Disposition should match acuity, response to treatment, social safety, and ongoing monitoring needs. For chronic cases, the workflow still applies, but the tempo changes. A patient with newly diagnosed type 2 diabetes requires diagnosis, initial treatment, education, cardiovascular risk modification, kidney assessment, eye referral, foot care, and follow-up. A patient with depression requires severity assessment, suicide risk evaluation, psychotherapy or medication options, adverse effect counseling, and follow-up. A patient with hypertension requires confirmation, risk assessment, lifestyle intervention, medication when indicated, and monitoring. These are management cases, not trivia cases. Practice the workflow out loud until it becomes automatic. During review, do not simply read the model answer. Reconstruct your sequence. Where did the first unsafe decision occur? Did you move the patient too late? Did you wait before treating? Did you treat before checking a contraindication? Did you forget reassessment? One corrected sequence can improve dozens of future cases. The final CCS risk is abandoning your system because of time pressure. On exam day, you need a short checklist that fits on your scratch paper and can be applied under stress. The checklist should not be a massive order set. It should be a cognitive guardrail. Begin every case with setting, acuity, and safety. Write “Where? Sick? Move?” at the top of your scratch space. This reminds you that location and triage come before diagnostic momentum. Then write “Stabilize before wait.” This prevents premature time advancement. Finally, write “Monitor, reassess, close.” This prevents cases from ending with an incomplete plan. Case endings can feel abrupt. Do not interpret every early ending as failure. Some simulations end when the core management tasks have been completed. Your job is to act safely and efficiently, not to fill every second. If the case continues, reassess. If it ends, move on mentally. Do not let one case contaminate the next. In the days before the exam, practice the interface enough that order entry is no longer novel. USMLE notes that examinees who do not practice the format and mechanics of CCS may be disadvantaged under standardized testing conditions. This is practical, not cosmetic. You should know how to place orders, advance time, respond to interval updates, and close a case without hunting through the interface. For final preparation, review your personal miss log. Do not only review high-yield diseases. Review high-yield behaviors. If you often forget pregnancy testing, put it on your reproductive-age checklist. If you forget pulse oximetry, attach it to dyspnea, sedation, sepsis, and respiratory cases. If you forget follow-up, make it part of every outpatient closure. If you advance time too quickly, force a “monitor first” pause. The safest CCS examinees are not perfect diagnosticians. They are consistent managers. They recognize acuity, protect the patient, order appropriate tests, start timely treatment, monitor response, and close the loop. That is the behavior Step 3 is designed to sample because Step 3 represents the final examination in the USMLE sequence and emphasizes readiness for unsupervised medical practice. Use this final mental script: “Right place, right urgency, right first treatment, right test, right monitoring, right follow-up.” If you can apply that script to every case, most avoidable CCS errors become much less likely. You will still encounter unfamiliar presentations, but your structure will keep you clinically safe while you reason through them. Medically reviewed by: Elena Ramirez, MD, MPH, Board-Certified Internal Medicine Physician.Why CCS Errors Happen Under Exam Pressure
Starting with labs only
Advancing time too early
Use a sequence
Mistake One: Missing Triage, Location, and Acuity
Acuity screen before orders
Mistake Two: Ordering Tests Without Stabilization
CCS scenario
Common mistake
Safer first move
Do before time advance
Hypotension with fever
Waiting for all labs before treatment
IV access, fluids, cultures when feasible, lactate, broad antibiotics
Recheck vitals and perfusion
Chest pain with diaphoresis
Troponin only
ECG, monitor, IV, aspirin if appropriate, symptom control
Assess ECG result and disposition
Altered mental status
CT first in every patient
Airway check, glucose, oxygenation, vitals, focused neurologic exam
Treat reversible threats
Severe dyspnea
Chest x-ray without respiratory support
Pulse oximetry, oxygen, bronchodilator or ventilatory support when indicated
Reassess work of breathing
Practice Step 3 management as an evolving patient-care loop.
Diagnosis is only the start of Step 3.
Mistake Three: Advancing Simulated Time Without Monitoring
Safe CCS time-advance flow
Mistake Four: Forgetting Contraindications, Counseling, and Prevention
Domain
Often forgotten
CCS prevention habit
Medication safety
Pregnancy status, allergies, renal function, bleeding risk
Check contraindications before high-risk drugs or imaging
Public health
Partner treatment, isolation, reporting, vaccination
Add infection-control and prevention orders when indicated
Chronic disease
Follow-up labs, adherence, lifestyle, adverse effects
Schedule monitoring after initiating treatment
Discharge
Return precautions, follow-up, education
Close with patient instructions and continuity plan
Mistake Five: Over-Ordering, Under-Ordering, and Losing the Case Thread
The seven-order filter
A Repeatable CCS Workflow for Every Case
Workflow step
Question to ask
Example actions
Triage
Can the patient safely remain here?
Move to ED, ICU, inpatient unit, or outpatient follow-up as appropriate
Stabilize
What can harm the patient now?
Oxygen, IV, fluids, monitor, glucose, airway support, urgent meds
Diagnose
What dangerous diagnoses must be ruled out?
ECG, imaging, CBC, CMP, cultures, pregnancy test, disease-specific tests
Treat
What therapy is indicated now?
Antibiotics, anticoagulation when safe, bronchodilators, insulin, procedures
Monitor
How will I know if the plan is working?
Serial vitals, pulse oximetry, telemetry, labs, urine output, symptom checks
Close
What must happen before discharge or admission?
Disposition, counseling, prevention, follow-up, return precautions
Rapid-Review Checklist for Exam Day
Rapid-Review Checklist
References
CCS Cases
Most common mistakes on Step 3 CCS cases and how to avoid them

For this CCS Cases problem
Practice Step 3 management as an evolving patient-care loop.
Move beyond knowing the diagnosis and practice what to do next as the patient changes.
Full access includes Step 1, Step 2 CK, Step 3, 135 CCS cases, analytics, auto-flashcards, and study planning.
Live case flow
Practice vitals, orders, labs, consults, and reassessment as the case evolves.
Order timing
Learn what must happen now, what can wait, and what loses value when late.
After-action review
See missed, late, unsafe, and unnecessary actions after each case.
Train Step 3 management
View Sample Cases
Full access is $27/month. Use it to practice this exact pattern while it is still fresh.
Mistake
Trap
Fix
From article to practice
Full access: $27/mo
Step 3 QBank135 CCS casesManagement reasoning
Monthly access. Cancel anytime. 7-day good-faith refund after baseline + 100 QBank questions or 5 CCS cases.
Management loop
Still missing the same kinds of questions?
Read why that happens.
Is the patient unstable? Stabilize and monitor before moving time.
Have time-sensitive tests or treatments been ordered? Review results when available.
Will the patient need reassessment soon? Advance in short intervals.
Is the patient stable with a chronic issue? Advance to appropriate follow-up.
Before case closure, update diagnosis, treatment, counseling, and disposition.