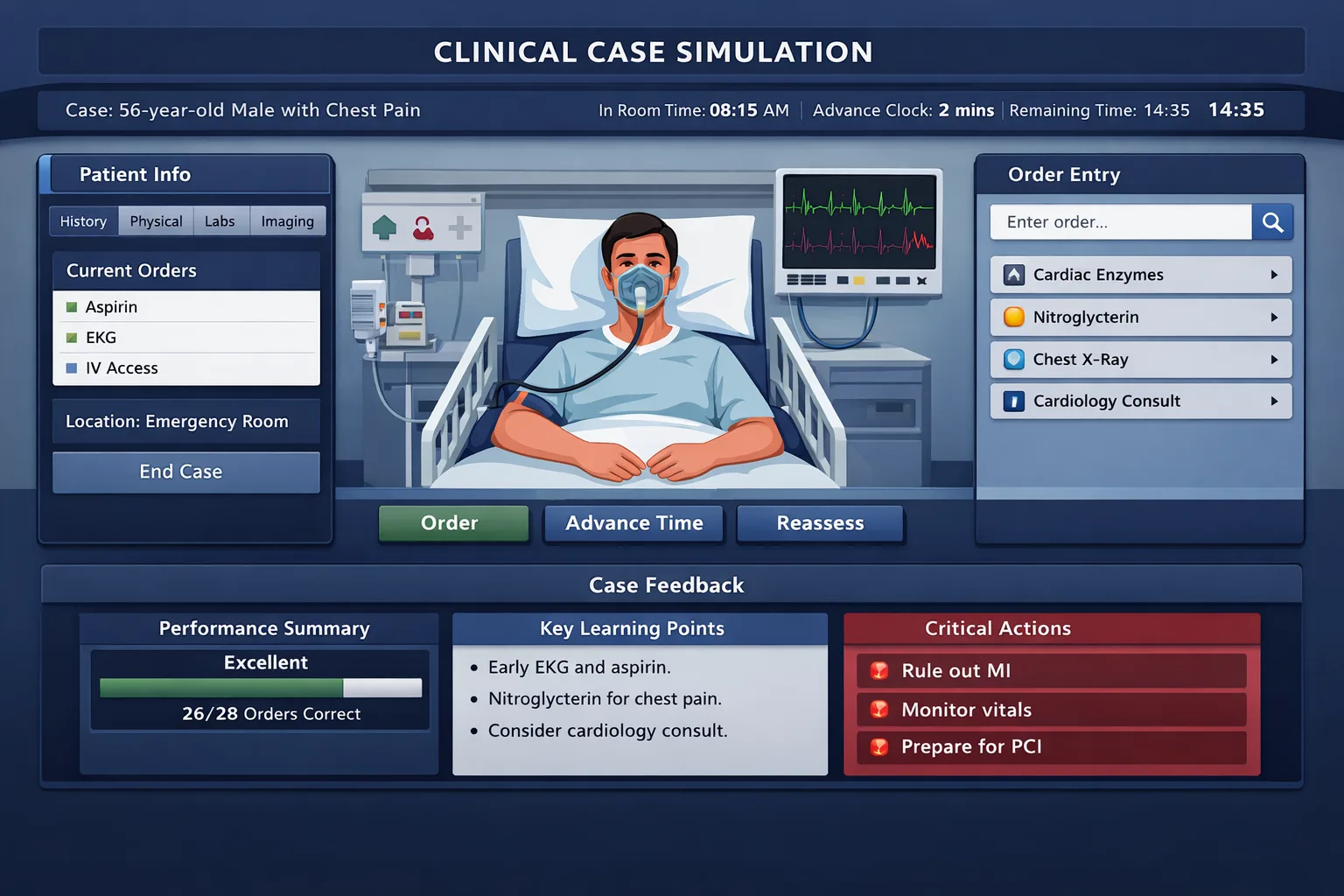
USMLE Step 3 CCS Strategy A strong Step 3 CCS orders checklist is not a memorized shotgun list. It is a repeatable clinical routine that helps you stabilize the patient, confirm the diagnosis, treat the active problem, prevent harm, and close the case with appropriate counseling. The goal is not to order everything. The goal is to never omit the order that a safe, independent physician would place in that setting. Computer-based case simulations test a different habit than multiple-choice questions. A vignette asks you to recognize the best answer among distractors. A CCS case asks you to practice medicine in sequence. You must decide where the patient belongs, what must happen now, what data are needed, which treatment should start before every result returns, and what follow-up protects the patient after the acute episode. That is why students who can answer Step 3 multiple-choice questions still lose points in CCS. They know the disease but do not have an order routine. The first mental shift is to stop treating CCS as a diagnostic puzzle only. Diagnosis matters, but management matters just as much. USMLE Step 3 CCS specifications include patient care diagnosis, laboratory and diagnostic studies, prognosis, treatment, health maintenance, surveillance, patient safety, and practice-based improvement. A case may reward prompt stabilization even before the final diagnosis is clear. Another case may punish unnecessary invasive orders, delayed antibiotics, failure to monitor a deteriorating patient, or forgetting pregnancy testing before imaging or medication exposure. The simulation rewards clinical prioritization. Think of every case as five linked decisions. First, identify acuity. A crashing patient in the emergency department, a febrile infant, chest pain with diaphoresis, hypotension, altered mental status, respiratory distress, active bleeding, suicidal intent, and toxic ingestion all require immediate stabilization. Second, select the right location. Office, emergency department, ward, ICU, and operating room are not interchangeable. Third, place core safety orders. Vitals, monitoring, IV access, oxygen when indicated, pain control, antiemetics, fluids, glucose, and airway support are not decorative. They demonstrate that you can keep the patient alive while you think. Fourth, order diagnostic studies that answer a clinical question. A CBC without a reason, a CT without a pregnancy check, or a broad autoimmune panel in a classic appendicitis case is inefficient. CCS rewards focused evaluation. Fifth, close the loop. Treatment is not complete when the patient improves. You still need disposition, diet or activity advice, medication counseling, return precautions, screening, vaccination, smoking cessation, or follow-up depending on the case. Many candidates remember the dramatic order and forget the quiet preventive order at the end. A good checklist therefore works like a cockpit routine. It does not replace judgment. It reduces omission under time pressure. On test day, you should not be inventing a fresh order structure for every case. You should be running a stable sequence: assess setting, stabilize, diagnose, treat, monitor, reassess, counsel, and follow up. The details change, but the spine stays the same. Recognizing pneumonia but forgetting pulse oximetry, blood cultures when septic, antibiotics, admission level, or smoking counseling. Order in layers: immediate safety, focused diagnosis, disease-specific treatment, monitoring, and prevention. Review every missed case by category: stabilizing order, diagnostic order, therapeutic order, monitoring order, or closing order. For Step 3, the most useful preparation is deliberate practice with timed simulations. Practicing the software matters because navigation errors consume cognitive bandwidth. The MDSteps CCS cases platform is built around timed orders, live vitals, and real physiology, so residents can practice the same sequence they want to execute on exam day. Use practice cases to build a personalized checklist from your own misses rather than copying a giant universal list. The first minute of a CCS case determines the rest of the encounter. Before ordering labs, decide whether the patient is stable, unstable, or potentially unstable. Stable patients can tolerate a full history and physical examination. Unstable patients need a brief focused examination and immediate orders. Potentially unstable patients may look well but carry a high-risk diagnosis, such as ectopic pregnancy, acute coronary syndrome, meningitis, sepsis, pulmonary embolism, stroke, torsion, diabetic ketoacidosis, or suicidal ideation with access to lethal means. Start with the setting. A patient with crushing chest pain in the emergency department should not be treated like an outpatient follow-up. A child with mild otitis media should not receive ICU-level interventions. A pregnant patient with abdominal pain, vaginal bleeding, syncope, or hypotension should trigger early pregnancy testing, type and screen when bleeding is present, pelvic ultrasound when indicated, and obstetric consultation when the case requires it. A confused or hypoxic patient often needs monitoring and a safer location before a complete diagnostic workup. The stabilizing order set should be specific to the patient, not automatic for everyone. Vitals are nearly universal. Pulse oximetry is appropriate for respiratory complaints, altered mental status, chest pain, sepsis, overdose, shock, and perioperative problems. Cardiac monitoring belongs in chest pain, syncope, arrhythmia, hyperkalemia, severe electrolyte disturbance, overdose, shock, and many ICU-level cases. Oxygen is appropriate for hypoxemia, respiratory distress, shock, major trauma, or peri-arrest states. It is not a substitute for diagnosing the cause of respiratory failure. IV access is an early order in emergency and inpatient cases where medications, fluids, contrast, blood, or rapid rescue therapy may be needed. In severe shock, two large-bore IV lines or central access may be reasonable. Fluids are not universal. Give isotonic fluids for hypovolemia, sepsis with hypotension, DKA, vomiting with dehydration, burns, and other volume-depleted states. Use caution in heart failure, renal failure, severe pulmonary edema, and cirrhosis. CCS rewards thoughtful treatment more than reflexive volume. Pain and nausea orders are often missed because learners worry they will obscure the diagnosis. In modern clinical care, severe pain should be treated while the diagnostic workup proceeds. Opioids may be appropriate for severe acute pain, but choose carefully in altered mental status, respiratory depression, and substance-related presentations. Antiemetics can support hydration and improve patient comfort. Fever control can be used, but it does not replace cultures, antibiotics, source control, or admission when infection is serious. Glucose is a high-yield safety order in altered mental status, seizure, diaphoresis, overdose, diabetes, alcohol use disorder, adrenal crisis, or unexplained weakness. A bedside glucose can immediately change management. Thiamine is appropriate before glucose in patients at high risk of Wernicke encephalopathy, especially chronic alcohol use disorder or severe malnutrition. Naloxone belongs in suspected opioid toxicity with respiratory depression. Do not give antidotes as decoration. Use them when the presentation supports the toxicologic syndrome. When a case begins with instability, do not spend several simulated hours gathering nonurgent data. Stabilize, reassess, and then advance time. The safest order sequence is often shorter than the most academically complete order list. Diagnostic orders in CCS should be driven by the leading diagnosis, dangerous alternatives, and treatment decisions. The common mistake is either under-ordering because the diagnosis feels obvious or over-ordering because the candidate lacks a differential. A focused diagnostic plan asks: What finding would confirm the diagnosis, rule out an emergency mimic, change management, affect disposition, or establish a baseline before treatment? Start with bedside tests when they can change immediate care. Fingerstick glucose is essential for altered mental status, seizure, diaphoresis, and any diabetic emergency. Urine pregnancy testing is high yield in reproductive-age patients with abdominal pain, pelvic pain, syncope, vaginal bleeding, nausea, medication exposure, or imaging needs. Pulse oximetry and ECG are also diagnostic in many cases, not just monitoring tools. In chest pain, syncope, hyperkalemia, overdose, and palpitations, an ECG often comes before broad laboratory interpretation. Core laboratory tests should match the setting. CBC can support infection, anemia, bleeding, malignancy, and inflammatory processes. A comprehensive metabolic panel helps in renal failure, liver disease, electrolyte disorders, dehydration, diabetes complications, and medication safety. Magnesium and phosphorus may matter in arrhythmias, alcohol use disorder, refeeding risk, DKA, and severe malnutrition. Coagulation studies are important before procedures, in liver disease, anticoagulant use, major bleeding, stroke thrombolysis evaluation, and disseminated intravascular coagulation concern. Urinalysis supports urinary infection, nephrolithiasis, nephritic syndromes, DKA, dehydration, and pregnancy-associated urinary disease. Use cultures correctly. Blood cultures should be ordered before antibiotics when this will not delay care in sepsis, meningitis, endocarditis, pyelonephritis with systemic toxicity, osteomyelitis, septic arthritis, and severe pneumonia. Urine cultures are useful in pyelonephritis, complicated urinary infection, pregnancy, recurrent infection, or suspected urosepsis. Wound, sputum, cerebrospinal fluid, or joint fluid cultures belong when the clinical source suggests them. Do not delay empiric antibiotics in a critically ill patient just because a culture order was missed. Place the culture order quickly and treat. Imaging should be targeted. Chest radiography is common for dyspnea, pneumonia, heart failure, pneumothorax, trauma, tuberculosis concern, and line placement. CT head is appropriate for focal neurologic deficit, acute severe headache with red flags, head trauma with risk features, altered mental status in selected settings, and anticoagulated trauma. CT abdomen and pelvis is useful for appendicitis, diverticulitis complications, obstruction, abscess, malignancy, and selected renal colic. Ultrasound is preferred for many biliary, pelvic, obstetric, testicular, and vascular questions. MRI is usually not the first move in unstable patients, but it is important in spinal cord compression, osteomyelitis, selected stroke pathways, and soft tissue or neurologic disease. Procedures are diagnostic orders too. Lumbar puncture can be necessary for meningitis or subarachnoid hemorrhage after appropriate imaging when indicated. Arthrocentesis matters in a hot swollen joint. Paracentesis is essential in suspected spontaneous bacterial peritonitis. Thoracentesis may be needed for unexplained pleural effusion. Do not forget that procedures also require safety planning: consent when relevant, coagulation review when appropriate, local anesthesia, culture or analysis of the sample, and monitoring afterward. Serology, endocrine testing, autoimmune panels, and tumor markers are lower-yield unless the case specifically calls for them. CCS is not a fishing expedition. In a classic panic attack presentation, you still consider ECG, glucose, thyroid disease, substance use, and safety assessment when clinically appropriate. In a classic acute coronary syndrome presentation, you do not need an autoimmune panel. The best diagnostic workup is broad enough to be safe and narrow enough to be clinically coherent. Practice the sequence: stabilize, diagnose, treat, reassess, and close the case without shotgun orders. Treatment timing is one of the highest-yield CCS skills. Many cases do not require you to wait for every confirmatory test. If the presentation supports a dangerous diagnosis, begin appropriate therapy while diagnostic confirmation proceeds. This is especially important in sepsis, meningitis, acute coronary syndrome, stroke, status epilepticus, anaphylaxis, DKA, asthma exacerbation, COPD exacerbation, hypertensive emergency, major trauma, gastrointestinal bleeding, ectopic pregnancy, testicular torsion, ovarian torsion, and acute angle-closure glaucoma. Antibiotics should be syndrome-specific. Suspected bacterial meningitis requires prompt empiric therapy, with adjunctive therapy when indicated, after blood cultures and lumbar puncture planning, unless imaging or instability delays lumbar puncture. Sepsis requires early antimicrobials when shock or high likelihood of infection is present, plus fluids when appropriate, lactate assessment, cultures, source evaluation, and admission. Pneumonia, pyelonephritis, cellulitis, diabetic foot infection, and intra-abdominal infection require coverage that matches severity and source. Avoid giving vancomycin and piperacillin-tazobactam to everyone. Broad coverage is justified in severe illness, resistant-organism risk, immunocompromise, health care exposure, or unclear source with shock. Cardiovascular cases need timely basics. In suspected acute coronary syndrome, think ECG, troponins, aspirin when not contraindicated, nitrates when appropriate, anticoagulation and P2Y12 therapy when indicated, statin therapy, oxygen only when hypoxemic or distressed, pain control, cardiology involvement, and reperfusion pathways for ST-elevation myocardial infarction. In unstable tachyarrhythmia, synchronized cardioversion is more important than debating oral rate control. In bradycardia with instability, pacing, atropine, vasopressors, and expert help may be needed. In heart failure with pulmonary edema, oxygen or ventilatory support, nitrates when blood pressure allows, diuresis, and precipitant evaluation matter. Respiratory treatment should be paired with monitoring. Asthma and COPD exacerbations require bronchodilators, systemic corticosteroids, oxygen titrated to clinical context, and escalation when severe. Pneumothorax requires needle decompression or chest tube when tension or large symptomatic disease is present. Pulmonary embolism may require anticoagulation, risk stratification, imaging, and thrombolysis or intervention in unstable massive PE. Do not forget contraindications to anticoagulation and the need for pregnancy-aware imaging decisions. Endocrine and metabolic cases reward order precision. DKA requires fluids, potassium assessment and replacement logic, insulin after potassium safety is addressed, glucose monitoring, electrolytes, anion gap tracking, and treatment of precipitant. Severe hyperkalemia with ECG changes requires membrane stabilization, intracellular shift therapy, potassium removal, and monitoring. Thyroid storm requires beta blockade, thionamide, iodine after thionamide, glucocorticoids, supportive care, and ICU-level monitoring. Adrenal crisis requires stress-dose steroids and fluids. Hypoglycemia requires dextrose and investigation of the cause. Surgical emergencies require consultation and nothing-by-mouth status. Appendicitis, bowel obstruction, perforation, acute cholecystitis with complications, ischemic bowel, testicular torsion, ovarian torsion, ectopic pregnancy rupture, compartment syndrome, epidural abscess with neurologic deficit, and necrotizing soft tissue infection should prompt early surgical or specialty consultation. Students often place the correct imaging order but forget NPO, IV fluids, analgesia, antibiotics when indicated, and operative consultation. In CCS, that is an incomplete plan. Airway, breathing, circulation, pain, nausea, glucose, monitors, location. Focused labs, imaging, cultures, procedure-based diagnosis. Disease-specific therapy before preventable deterioration. Advance time only after orders are placed and monitoring is active. Use treatment orders as proof of clinical judgment. The case should show that you identified risk, started appropriate therapy, avoided contraindicated therapy, and escalated care when needed. CCS cases evolve. A patient can improve, worsen, or fail to respond. Monitoring orders show that you are not practicing one-time medicine. They also protect you from advancing simulated time while an unstable patient is unobserved. The most commonly missed monitoring orders are repeat vital signs, continuous pulse oximetry, cardiac monitoring, serial neurologic checks, strict intake and output, urine output, repeat glucose, repeat electrolytes, repeat troponins, repeat lactate, and fetal monitoring when pregnancy-related emergencies require it. Monitoring should match the disease. Acute coronary syndrome requires serial ECGs and troponins, telemetry, blood pressure monitoring, and reassessment of pain. DKA requires frequent glucose, potassium, bicarbonate, anion gap, and volume status checks. Sepsis requires blood pressure, urine output, mental status, lactate reassessment when elevated, source control planning, and ICU escalation if shock persists. Stroke requires neurologic checks, blood pressure strategy, swallow evaluation before oral intake, and rehabilitation planning. Asthma requires respiratory status, oxygen saturation, peak flow when useful, and escalation for fatigue or poor response. Diet and activity orders are easy points when used correctly. NPO belongs in surgical emergencies, bowel obstruction, pancreatitis when severe or vomiting, aspiration risk, procedural sedation, and airway-risk situations. Cardiac diet, diabetic diet, renal diet, or regular diet can be appropriate after stabilization depending on the condition. Bed rest, fall precautions, seizure precautions, aspiration precautions, suicide precautions, contact precautions, droplet precautions, and isolation orders are not glamorous, but they can be central to patient safety. Disposition is not just admission versus discharge. Ask where the patient can safely receive care. ICU is appropriate for shock, respiratory failure, need for vasopressors, severe DKA with instability, severe sepsis, airway risk, status epilepticus, severe GI bleeding, malignant arrhythmia, and close neurologic monitoring. The ward may be enough for moderate pneumonia requiring IV antibiotics in a stable patient. Observation can fit selected chest pain, syncope, or dehydration cases. Outpatient care is appropriate only when dangerous diagnoses are excluded, symptoms are controlled, follow-up is reliable, and return precautions are clear. Consultations should answer a clinical need. Cardiology for STEMI, unstable arrhythmia, advanced heart failure, or high-risk ACS. Surgery for appendicitis, obstruction, perforation, abscess drainage, ischemia, torsion, and necrotizing infection. Obstetrics for ectopic pregnancy, severe preeclampsia, third-trimester bleeding, fetal distress, and complicated pregnancy. Psychiatry for suicidality, homicidality, psychosis with safety concerns, severe mania, or inability to care for self. Infectious disease is useful for complex antimicrobial decisions, endocarditis, opportunistic infection, and resistant organisms. Nephrology for dialysis indications, severe renal failure, refractory hyperkalemia, and complex electrolyte problems. Reassessment is where many CCS cases turn. After placing orders, advance time in clinically reasonable increments and review results. If a patient improves, de-escalate appropriately, transition to oral therapy when indicated, discharge safely, and add follow-up. If the patient worsens, do not keep advancing time. Escalate location, broaden differential, repeat focused examination, add monitoring, call consultants, and adjust therapy. The case is testing whether you respond to feedback. In practice sessions, pause after every case and ask one question: Did I manage the patient over time, or did I only make the diagnosis? That distinction is central to Step 3 CCS performance. End-of-case orders are not filler. They often represent the difference between treating the acute complaint and practicing independent medicine. Step 3 expects attention to health maintenance, disease prevention, communication, professionalism, systems-based practice, and patient safety. In CCS, that can mean screening, vaccination, medication reconciliation, counseling, follow-up, home safety, return precautions, and documentation of patient education. For outpatient cases, prevention can be the main task. Hypertension, diabetes, obesity, smoking, alcohol use, depression, anxiety, intimate partner violence, sexually transmitted infection risk, contraception, prenatal care, and cancer screening may be central. Do not turn every office visit into a hospital workup. Instead, identify age-appropriate screening, risk-factor counseling, medication adherence, adverse effects, and follow-up intervals. A patient with uncontrolled diabetes may need A1c, urine albumin-creatinine ratio, lipid management, eye referral, foot examination, vaccination review, nutrition counseling, and hypoglycemia education. A smoker with COPD symptoms may need spirometry, inhaler therapy, vaccination review, smoking cessation, and oxygen assessment when severe. For inpatient and emergency cases, prevention usually appears after stabilization. A patient admitted with myocardial infarction may need smoking cessation, cardiac rehabilitation, statin therapy, antiplatelet education, medication adherence counseling, and follow-up. A patient treated for DKA needs sick-day rules, insulin education, glucose monitoring, precipitant treatment, and outpatient diabetes follow-up. A patient with a fragility fracture needs pain control and orthopedic care, but also fall-risk evaluation, vitamin D and calcium discussion when appropriate, bone health workup, and home safety planning. A patient with alcohol withdrawal needs thiamine, benzodiazepine-based management when indicated, withdrawal monitoring, counseling, and referral for treatment after stabilization. Vaccination orders should be realistic. Adult immunization decisions depend on age, pregnancy, chronic disease, immunocompromise, prior vaccination, occupation, and risk factors. Influenza vaccination, COVID-19 vaccination guidance, pneumococcal vaccination, hepatitis B vaccination, shingles vaccination, Tdap or Td boosters, RSV vaccination in eligible groups, and HPV vaccination in appropriate age groups are common preventive themes. In CCS, you do not need to reproduce an entire schedule, but you should recognize when vaccine review belongs in chronic disease, pregnancy, older adult care, immunocompromise, asplenia, liver disease, diabetes, and smoking-related visits. Counseling should match the diagnosis. Asthma requires inhaler technique and trigger avoidance. GERD requires lifestyle counseling and alarm symptom follow-up. Kidney stones require hydration advice and stone analysis when appropriate. Sexually transmitted infection cases require partner notification, abstinence until treatment completion when appropriate, and screening for co-infections. Psychiatric cases require safety planning, removal of lethal means, crisis resources, and follow-up. Pediatric cases often require caregiver education, hydration instructions, fever guidance, and return precautions. Safety orders are easy to overlook. Fall precautions, aspiration precautions, seizure precautions, suicide precautions, domestic violence safety planning, anticoagulation counseling, pregnancy counseling, medication interaction review, renal-dose adjustment, allergy checks, and follow-up of pending tests all show mature care. These orders are especially important because CCS cases can end early when the patient improves. If you forget prevention and safety until the final seconds, you may not have enough time to enter them. MDSteps can help convert missed CCS orders into flashcards and study tasks when learners use the broader Step 3 preparation workflow. The practical advantage is not memorizing more facts. It is seeing patterns in what you personally omit, then drilling those omissions until they become automatic. The best CCS checklist is short enough to use under pressure. A long list of every possible order becomes noise. Use a universal skeleton, then attach disease-specific modules. The universal skeleton is location, vitals, focused exam, stabilization, diagnostic confirmation, treatment, monitoring, consultation, disposition, and closing care. Disease modules then remind you of orders that are easy to miss in a specific presentation. For chest pain, think ECG immediately, aspirin if not contraindicated, troponins, cardiac monitor, IV access, chest radiograph when indicated, nitrates if appropriate, anticoagulation and reperfusion pathway when ACS is likely, and oxygen only when hypoxemic or in respiratory distress. Do not forget contraindications to nitrates, bleeding risk, aortic dissection clues, pulmonary embolism, pericarditis, pneumothorax, and esophageal rupture. The trap is anchoring on myocardial infarction and missing the dangerous mimic. For abdominal pain, begin with pregnancy testing when applicable, vitals, pain control, antiemetic therapy, CBC, metabolic panel, urinalysis, liver enzymes and lipase when indicated, imaging tailored to location, NPO when surgical disease is possible, IV fluids for dehydration or sepsis, antibiotics for intra-abdominal infection, and surgical or gynecologic consultation when needed. Do not forget testicular torsion in lower abdominal pain in males, ectopic pregnancy in reproductive-age females, AAA in older patients, and ischemic bowel in pain out of proportion to examination. For dyspnea, order pulse oximetry, oxygen if hypoxemic, chest radiograph, ECG, bronchodilator therapy when bronchospasm is present, diuretics and nitrates when pulmonary edema is likely and blood pressure allows, antibiotics when pneumonia is likely, anticoagulation or imaging when PE is likely, and ventilatory support when fatigue or respiratory failure develops. Do not forget that normal oxygen saturation does not exclude serious disease, especially early PE or metabolic acidosis. For fever and infection, ask whether the patient is toxic. Stable outpatient infections may need targeted tests and oral therapy. Sepsis requires IV access, fluids when appropriate, lactate, cultures, early antibiotics, source evaluation, urine output, and admission level. Meningitis, endocarditis, epidural abscess, septic arthritis, necrotizing fasciitis, and febrile neutropenia require urgent, specific pathways. Do not let a broad infection label replace source control. For neurologic cases, check glucose first when mental status is altered. Stroke requires last-known-well timing, CT head, neurologic assessment, blood pressure strategy, glucose, ECG, swallow screen, reperfusion evaluation, and stroke-team involvement when available. Seizure requires safety, benzodiazepines for ongoing seizure, antiseizure therapy for status epilepticus, glucose, electrolytes, toxicology when relevant, pregnancy testing when applicable, and imaging when indicated. Headache requires red-flag triage: thunderclap onset, neurologic deficits, papilledema, fever, pregnancy, cancer, immunosuppression, anticoagulation, and trauma. For psychiatric and behavioral cases, never forget safety. Suicidal ideation requires suicide precautions, removal of lethal means, psychiatric evaluation, substance assessment, medical causes when appropriate, and safe disposition. Agitation requires verbal de-escalation, safety, glucose, toxicology or medical evaluation when indicated, and medication only when necessary for safety. Intoxication and withdrawal require airway risk, vitals, glucose, thiamine in high-risk patients, benzodiazepines for alcohol withdrawal when indicated, and monitoring. The final goal is to convert your knowledge into a reliable exam-day routine. Before every CCS session, write a short framework on your scratch surface if allowed by your testing center instructions. Keep it brief. A useful version is: site, acuity, vitals, monitors, IV or oxygen when needed, glucose or pregnancy when relevant, focused diagnostics, targeted treatment, reassess, disposition, prevention, and follow-up. That sequence covers most missed-order categories without pushing you toward indiscriminate ordering. During the case, read the location and chief complaint carefully. A patient in the office with chronic fatigue is not the same as a patient in the emergency department with hypotension. Decide whether you need a complete physical examination or a focused examination. In a sick patient, use a focused examination and stabilize first. In a stable patient, a complete examination may reveal clues that prevent unnecessary testing. Never advance time after a dangerous initial presentation until monitoring and urgent treatment orders are active. Use result review as a trigger for action. If potassium is dangerously high, treat it. If lactate is elevated with infection concern, escalate sepsis management. If troponin rises, update the ACS pathway. If CT shows appendicitis, call surgery, keep the patient NPO, give antibiotics when indicated, and manage pain. If the case improves, do not stop thinking. Add discharge counseling, preventive care, and follow-up. If the case worsens, do not keep ordering random labs. Reassess the patient, broaden the differential, escalate care, and consult appropriately. Practice cases should be reviewed in a structured way. Do not only ask whether you diagnosed correctly. Ask which category you missed. Stabilization misses include no monitor, no oxygen when hypoxemic, no IV access, no glucose check, no pregnancy test, no pain control, or no isolation precautions. Diagnostic misses include no ECG, no cultures, no source imaging, no lumbar puncture, or no procedure. Treatment misses include delayed antibiotics, no fluids when indicated, no anticoagulation when appropriate, no insulin protocol, or no surgical consultation. Monitoring misses include no serial labs, no telemetry, no neuro checks, no urine output, or no repeat vitals. Closing misses include no counseling, vaccination review, return precautions, or follow-up. Build flashcards from omission categories, not from entire cases. A card that says “febrile hypotensive patient” should prompt lactate, cultures, antibiotics, fluids when indicated, urine output, and source control. A card that says “reproductive-age abdominal pain” should prompt pregnancy test, ectopic consideration, pelvic or abdominal imaging as indicated, pain control, and gynecology or surgery when needed. This is how a checklist becomes a clinical reflex. A strong checklist should make you calmer, not more rigid. CCS cases reward flexible clinical reasoning built on a consistent safety structure. Practice with timed simulations, review your missed orders, and refine your personal checklist until it fits on one page. For broader case reasoning, review the MDSteps sample question breakdown and apply the same stabilize, diagnose, treat, and reassess logic to both CCS and multiple-choice questions. Medically reviewed by: Daniel R. Hoffman, MD, FACPStep 3 CCS Orders Checklist: Do Not Forget These Orders
Why CCS Orders Are Different From Multiple-Choice Reasoning
The exam trap
The safe habit
The study method
The First 60 Seconds: Location, Acuity, and Stabilization
Clinical cue
Do not forget
Common omission
Chest pain, syncope, palpitations
Vitals, ECG, cardiac monitor, pulse oximetry, IV access
Ordering troponin but forgetting immediate ECG or monitoring
Dyspnea or hypoxemia
Pulse oximetry, oxygen if hypoxemic, chest imaging, ABG or VBG when severe
Treating asthma, COPD, CHF, or PE without monitoring response
Fever with hypotension or confusion
IV access, fluids when appropriate, lactate, cultures, antibiotics, admission level
Waiting for every test before starting treatment
Altered mental status
Glucose, pulse oximetry, toxicology when indicated, CT head when indicated
Skipping reversible causes such as hypoglycemia or hypoxia
Pregnancy possibility
Pregnancy test before teratogenic medication or ionizing imaging when feasible
Ordering CT or contraindicated drugs without checking pregnancy status
Diagnostic Orders You Should Not Forget
Red-flag diagnostic omissions
Stop treating CCS like a memorized order list.
Correct orders still need the right order.
Treatment Orders: Act Before the Case Drifts
Stabilize
Confirm
Treat
Reassess
Monitoring, Reassessment, and Disposition Orders
Case pattern
Monitoring often needed
Disposition clue
ACS or arrhythmia
Telemetry, serial ECG, serial troponin, blood pressure
Observation, ward, cath lab, or ICU based on instability
Sepsis or shock
Vitals, urine output, lactate, mental status, cultures, response to fluids
ICU if persistent hypotension, vasopressors, or organ failure
DKA or severe electrolytes
Glucose, potassium, bicarbonate, anion gap, urine output
ICU or step-down if severe, unstable, or needing insulin infusion
Neurologic emergency
Neuro checks, airway risk, swallow screen, BP targets
Stroke unit or ICU depending on severity and intervention
Preventive, Counseling, and Safety Orders at the End
High-yield closing orders
A Practical Order Checklist by Case Type
Presentation
Orders not to miss
Board-style trap
Chest pain
ECG, monitor, troponins, aspirin, IV access, reperfusion planning if STEMI
Missing dissection, PE, pneumothorax, or nitrate contraindication
Abdominal pain
Pregnancy test, pain control, targeted labs, imaging, NPO, surgery consult when needed
Forgetting ectopic pregnancy, torsion, AAA, or ischemic bowel
Dyspnea
Pulse oximetry, oxygen if needed, ECG, chest radiograph, disease-specific treatment
Treating all wheeze as asthma or all edema as CHF
Sepsis pattern
IV access, fluids if indicated, lactate, cultures, antibiotics, source control
Waiting too long for confirmatory results before treatment
Altered mental status
Glucose, oxygenation, vitals, medication review, toxicology when indicated, CT when indicated
Missing hypoglycemia, hypoxia, sepsis, overdose, or intracranial bleeding
Rapid-Review Checklist for Exam Day
Exam-Day Essentials
References
CCS Cases
Step 3 CCS cases checklist: orders you should not forget

For this CCS Cases problem
Stop treating CCS like a memorized order list.
Practice the sequence: stabilize, diagnose, treat, reassess, and close the case without shotgun orders.
Full access includes Step 1, Step 2 CK, Step 3, 135 CCS cases, analytics, auto-flashcards, and study planning.
Live case flow
Practice vitals, orders, labs, consults, and reassessment as the case evolves.
Order timing
Learn what must happen now, what can wait, and what loses value when late.
After-action review
See missed, late, unsafe, and unnecessary actions after each case.
Practice CCS order sequencing
View Sample Cases
Full access is $27/month. Use it to practice this exact pattern while it is still fresh.
From article to practice
Full access: $27/mo
135 CCS casesOrder timing reviewAfter-action feedback
Monthly access. Cancel anytime. 7-day good-faith refund after baseline + 100 QBank questions or 5 CCS cases.
CCS sequencing
Still missing the same kinds of questions?
Read why that happens.
1
2
3
4