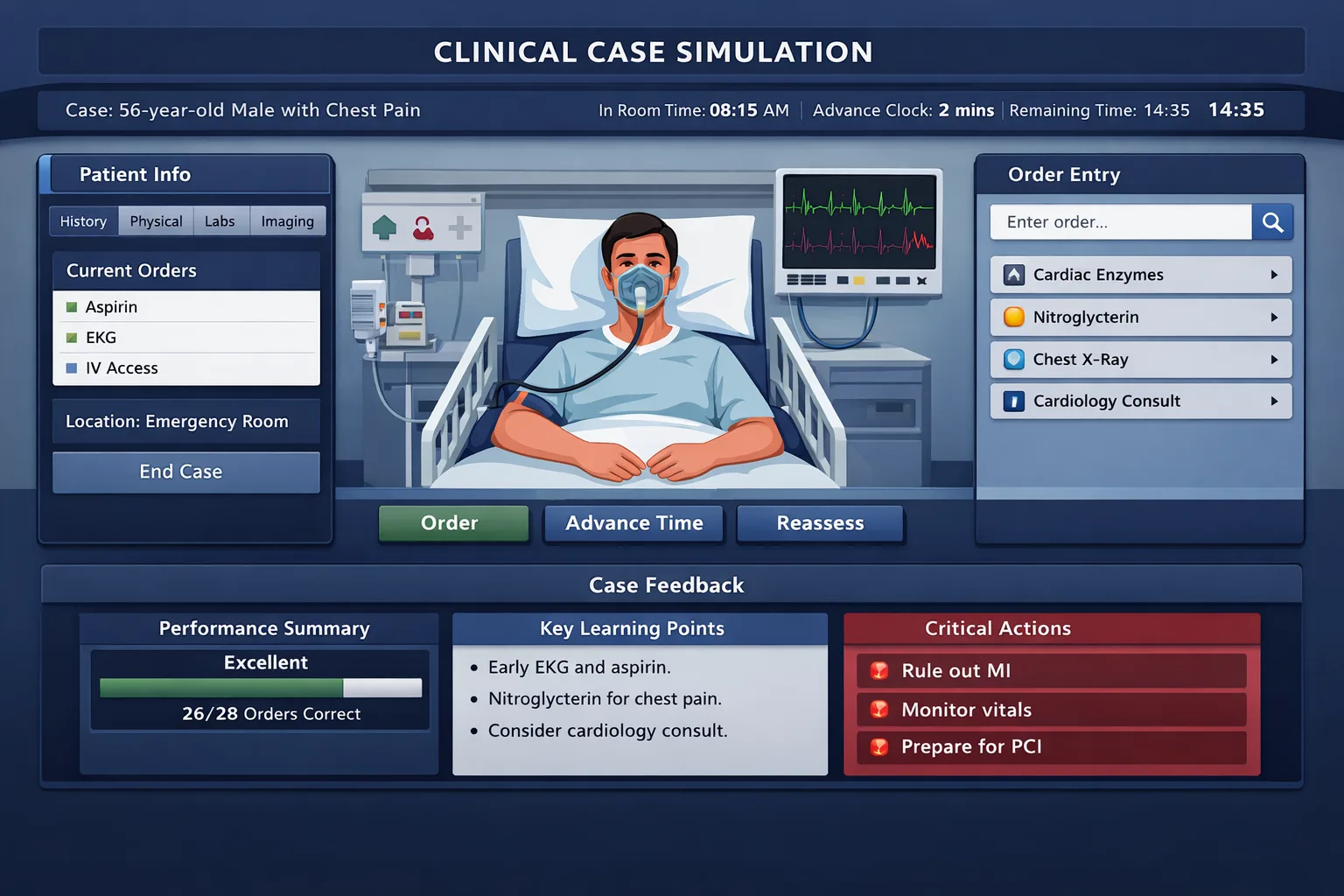
Computer-based case simulations are not ordinary multiple-choice questions with a different interface. They are dynamic patient-care simulations. The examinee must decide what to ask, what to examine, what to order, when to advance time, when to reassess, when to treat, and when to close the encounter. For many international medical graduates, the medical knowledge is present, but the scoring challenge comes from translating that knowledge into United States-style, timed, systems-aware management. The most important shift is moving from diagnosis-first thinking to safety-first management. In a written exam, the correct answer may be the most likely diagnosis. In CCS, the case rewards a sequence. Stabilize dangerous physiology, collect focused data, start time-sensitive treatment, monitor response, narrow the diagnosis, change location when needed, and document preventive or counseling actions before closure. A patient with chest pain is not simply a myocardial infarction question. It is a decision about oxygen only when indicated, cardiac monitoring, intravenous access, ECG, troponin, aspirin when appropriate, anticoagulation or reperfusion logic, admission level, follow-up testing, and counseling. IMGs often have three predictable friction points. First, many have trained in environments where broad panels are ordered by default because cost, availability, or local workflow differs. CCS requires purposeful breadth. Missing a critical order can hurt, but ordering everything without a clinical reason can also signal poor management. Second, transition-of-care actions may feel unfamiliar. The simulation expects attention to emergency department, office, inpatient ward, intensive care, operating room, and discharge decisions. Third, preventive care and counseling may not be emphasized equally across training systems. Vaccination, smoking cessation, diet, return precautions, safe sex counseling, medication adherence, and follow-up can matter when the case is stable. The practical goal is not to memorize one universal order list. The goal is to build reusable case scripts. Each script should answer four questions: is the patient unstable, what diagnosis can kill quickly, what test changes management now, and what treatment should not wait for every result. That script must then be rehearsed until it can be performed under time pressure. CCS is partly knowledge, partly sequencing, and partly interface fluency. Step 3 is the final examination in the USMLE sequence and is designed around independent, unsupervised practice. The exam is divided into Foundations of Independent Practice on Day 1 and Advanced Clinical Medicine on Day 2. CCS cases appear on Day 2, after multiple-choice blocks. The official exam resources describe CCS cases as interactive simulations that assess diagnosis, treatment, and monitoring. For testing beginning with the 2026 software update, Step 3 uses shorter multiple-choice blocks while retaining 13 to 14 case simulations on Day 2. That structure has two implications for IMGs. First, CCS preparation cannot be postponed until the final weekend. By the time you reach the simulations on Day 2, fatigue is real. Order entry must be automatic enough that you are not using working memory to remember where each action belongs. Second, you must practice with a case interface, not only read cases. The official USMLE materials state that examinees who do not practice the format and mechanics of CCS are likely to be at a disadvantage. That warning should guide your schedule. CCS cases use simulated time. Real clock time and patient time are different. You may advance simulated time to receive results, observe clinical changes, or move toward follow-up. The patient can improve, worsen, or remain unchanged based on the disease and your management. This is where many otherwise strong test takers lose points. They order the right tests but fail to reassess. They treat correctly but leave the patient in the wrong setting. They admit appropriately but do not monitor the problem they are treating. For IMGs, the safest preparation model is a three-layer model. Layer one is interface fluency: order entry, time advancement, interval history, physical examination, location change, and case closure. Layer two is clinical scripts: chest pain, dyspnea, abdominal pain, neurologic deficit, sepsis, endocrine emergencies, obstetric or gynecologic complaints, pediatrics, psychiatry, and office prevention. Layer three is scoring discipline: avoid harmful actions, do not delay urgent treatment, document reassessment, and finish with disposition plus patient education. A reliable CCS approach begins before the diagnosis is certain. Start with the stem, location, age, vital signs, and chief concern. Ask whether the patient is unstable. Instability includes airway compromise, hypoxemia, shock, altered mental status, severe pain with toxic appearance, active bleeding, focal neurologic deficit, peritonitis, suicidal or homicidal risk, and obstetric emergency signs. When instability is present, the first orders should protect life before they prove the diagnosis. A useful framework is SODA: Stabilize, Order, Diagnose, Act again. Stabilize means place the patient in the correct setting, obtain intravenous access when appropriate, monitor cardiac rhythm or oxygen saturation when indicated, give oxygen when hypoxemic, administer fluids or blood products when clinically justified, and manage immediate threats. Order means choose focused tests that will change management. Diagnose means interpret results in context, not in isolation. Act again means adjust therapy, consult, move location, or discharge with follow-up. History and physical examination should be targeted. In the emergency department, do not spend simulated time collecting a complete social history before treating an unstable patient. In an office case, do not skip the history elements that define risk, screening eligibility, medication safety, pregnancy possibility, or adherence. CCS rewards clinical context. A young patient with pleuritic chest pain and tachycardia needs a different script from an older patient with crushing substernal pain and diaphoresis. Both may start with chest pain, but the danger list differs. After initial orders, reassessment is the most common missed habit. A case should not be treated as a static checklist. If you give fluids, reassess blood pressure, urine output when relevant, lung exam in patients at risk of overload, and symptoms. If you treat asthma, reassess respiratory rate, oxygen saturation, wheezing, work of breathing, and peak flow if appropriate. If you start antibiotics for sepsis, reassess vitals and cultures while also controlling the source when indicated. Practicing this framework with live cases is more efficient than reading long lists of orders. MDSteps Step 3 CCS practice includes timed orders, changing vitals, real case progression, and after-action feedback, which helps IMGs convert clinical knowledge into the exact sequence CCS requires. Practice live cases where timing, reassessment, stabilization, order value, and closure matter. MDSteps helps you see what was missed, late, unsafe, unnecessary, or done in the wrong sequence. Order sets are useful only when they are tied to a reason. The dangerous habit is memorizing hundreds of orders without knowing when to use them. CCS is not asking whether you can order every test in a hospital. It is asking whether your management is safe, efficient, and responsive. The best order sets are short, presentation based, and separated into initial, conditional, and closure orders. For chest pain, the initial frame usually includes vital reassessment, ECG, cardiac monitoring, troponin, aspirin when not contraindicated, and risk-based therapy. For dyspnea, focus on oxygenation, pulse oximetry, chest imaging when appropriate, ECG when cardiopulmonary causes are plausible, bronchodilators for obstructive disease, diuretics for pulmonary edema, or anticoagulation workup for suspected pulmonary embolism. For fever with hypotension, the frame becomes sepsis: cultures when feasible, broad empiric antibiotics, lactate when appropriate, fluids, source evaluation, and escalation if shock persists. For abdominal pain, avoid anchoring. The CCS trap is ordering pain medication and imaging while missing pregnancy testing, peritoneal signs, unstable vitals, surgical consultation, or bowel ischemia clues. For neurologic deficits, timing is central. Glucose, neurologic examination, head imaging logic, stroke window thinking, blood pressure strategy, swallow precautions, and admission level should appear early when the presentation supports stroke. For altered mental status, remember glucose, oxygenation, infection, medication or toxin exposure, trauma, seizure, metabolic derangement, and intracranial disease. Office cases require a different rhythm. You still need diagnosis and management, but the scoring opportunity often includes prevention. Diabetes follow-up should include A1c logic, kidney monitoring, eye and foot care, blood pressure and lipid risk, lifestyle counseling, and medication adherence. Hypertension follow-up should include measurement confirmation, secondary causes when suggested, end-organ risk, lifestyle, medication selection, and follow-up timing. Depression should include safety assessment, functional impairment, substance use, medication or therapy planning, and follow-up. The first common mistake is treating CCS like an oral exam. Some IMGs overexplain the diagnosis mentally but underperform the actions. The computer does not know that you considered pulmonary embolism unless your orders show that you evaluated or treated it appropriately. Convert reasoning into visible management. The second mistake is ordering broad tests before addressing abnormal vital signs. A patient with hypotension, hypoxemia, severe altered mental status, or active bleeding needs immediate stabilization. Diagnostic completeness should not delay urgent care. In CCS, this is especially important because simulated time can pass and the patient can deteriorate. The third mistake is failing to change location. Many international clinical settings have different thresholds for intensive care, observation, or outpatient management. CCS expects the setting to match acuity. A patient needing vasopressors, mechanical ventilation, severe DKA monitoring, unstable arrhythmia care, or evolving sepsis should not remain in a routine office or unmonitored floor environment. Conversely, stable outpatient cases should not be admitted reflexively. The fourth mistake is overusing invasive procedures or consultations. Consults are appropriate when they change management, such as surgery for acute abdomen, cardiology for high-risk ACS, psychiatry for unsafe suicidality, obstetrics for pregnancy emergencies, or intensive care for shock. They should not replace your initial stabilization. Similarly, procedures should match the diagnosis and setting. The exam is not impressed by aggression when conservative, guideline-consistent management is safer. The fifth mistake is forgetting negative actions. Do not give contraindicated medications. Do not discharge unstable patients. Do not advance time after ordering treatment for a dangerous condition without reassessing. Do not ignore pregnancy status when ordering teratogenic medications or imaging that requires risk consideration. Do not forget allergies, renal function, anticoagulation status, and medication interactions when clinically relevant. The sixth mistake is neglecting closure. At the end of a stable case, the patient may need counseling, follow-up, medication instructions, return precautions, preventive screening, or rehabilitation planning. These actions should be focused. A patient with new diabetes needs education, monitoring, and follow-up. A patient treated for pneumonia needs medication adherence instructions and warning signs. A patient with depression needs safety planning and follow-up. A strong plan should combine case volume, deliberate review, and spaced correction. Passive reading feels efficient but does not build case execution. Retrieval practice works because it forces you to produce the next step before seeing the answer. Spaced review helps convert the same missed pattern into a durable habit. For CCS, this means repeating the exact action you missed, not merely rereading an explanation. Week 1 should focus on mechanics and common emergency scripts. Complete cases slowly at first. Pause after the stem and write the first five actions you expect. Then run the case and compare. Build scripts for chest pain, dyspnea, sepsis, abdominal pain, altered mental status, neurologic deficit, DKA, asthma or COPD, hypertensive emergency, trauma, and suicidal ideation. Your aim is not speed yet. Your aim is safe sequencing. Week 2 should add outpatient and chronic disease cases. Many IMGs overprepare for dramatic emergencies and underprepare for stable office management. Practice diabetes, hypertension, preventive care, prenatal complaints, pediatric fever, back pain, depression, substance use, anticoagulation issues, and medication adverse effects. Add counseling and follow-up orders only after diagnosis and treatment are safe. Week 3 should become timed. Run mixed cases without knowing the category. After each case, classify every miss as one of five types: stabilization, diagnostic testing, treatment, reassessment, or disposition. This classification is more useful than a raw score because it tells you what habit failed. If you repeatedly miss reassessment, add a mandatory rule: after every treatment and time advance, check vitals and focused symptoms. Week 4 should simulate exam fatigue. Put CCS after multiple-choice blocks or after a long clinical day. Practice decision quality when tired. Review only your highest-yield miss log. Avoid adding new resources late unless a gap is obvious. The final week is for tightening scripts, not expanding chaos. MDSteps can support this phase by pairing live vitals CCS cases with an analytics dashboard, automatic study planning, an adaptive QBank with more than 9000 questions, and flashcard decks generated from missed concepts that can be exported to Anki. Use those tools to identify whether your CCS mistakes are knowledge gaps, timing gaps, or repeat execution habits. The most valuable learning happens after the case ends. A weak review asks, “What was the diagnosis?” A strong review asks, “Where did my management stop matching the patient’s risk?” The second question is better because CCS scoring depends on management, not just recognition. Create a short miss log and keep it structured. Start with stabilization. Did the patient have abnormal vital signs or a dangerous presentation? Did you address airway, breathing, circulation, mental status, pain, bleeding, or unsafe psychiatric risk? If not, write the missed action as a future trigger. For example: “Tachycardia plus fever plus hypotension means sepsis frame before full diagnostic certainty.” Next review diagnostic testing. Separate essential tests from nice-to-have tests. Essential tests are those that change immediate treatment, rule out dangerous diagnoses, or guide disposition. Nice-to-have tests may be appropriate later but should not crowd the first minute. A broad order panel may hide that you never ordered the one test that mattered early. Then review treatment. Ask whether treatment was too early, too late, or wrong for the likely diagnosis. Early treatment is good when delay is harmful, as in suspected sepsis, anaphylaxis, severe asthma, status epilepticus, hypoglycemia, or certain ACS pathways. Early treatment is unsafe when the action is invasive, contraindicated, or unsupported by the case. Reassessment comes next. This is where a simple habit can improve many cases. After any meaningful intervention, check whether the patient improved. After advancing time, look at vitals and symptoms. After receiving results, decide whether the plan changes. The patient’s response is not decoration. It is the simulation’s feedback loop. Finally, review disposition and closure. Did you place the patient in the correct setting? Did you discharge only when stable? Did you provide follow-up, return precautions, counseling, or prevention when appropriate? The end of the case should show that you can hand off or complete care safely. On exam day, your goal is not brilliance. It is safe, consistent management. Read the stem, identify location, scan vital signs, and decide whether the patient is unstable. If unstable, stabilize before chasing diagnostic elegance. If stable, collect focused history and physical information, order targeted tests, treat based on risk, advance time carefully, and reassess. Use the final minutes of each case wisely. Closure orders should not replace urgent care, but they can complete a stable encounter. Think about medication counseling, lifestyle counseling, smoking cessation, vaccine or screening needs, follow-up, return precautions, physical therapy, home safety, or specialist follow-up when clinically justified. Avoid generic counseling floods. The best closure actions are specific to the case. Expect fatigue on Day 2. The multiple-choice blocks come before CCS, so build a simple reset ritual before the cases begin. Take an authorized break when available, eat something predictable, hydrate, and remind yourself of the sequence: stabilize, order, diagnose, act again. During each case, do not panic if one result is not what you expected. CCS cases often reward adjustment. A patient who worsens is not an automatic failure if you recognize the change and respond safely. For IMGs, the best final preparation is not trying to imitate another person’s order list. It is building a disciplined clinical reflex that works across unfamiliar cases. Know the interface. Practice timed cases. Review misses by category. Rehearse transitions of care. Treat unstable patients first. Reassess after every meaningful intervention. When your practice looks like that, Step 3 CCS becomes less mysterious and more like the clinical work it is designed to simulate. Medically reviewed by: Jonathan R. Feldman, MD, Internal Medicine.Why CCS feels different for international graduates
Understand the current Step 3 CCS format before building a plan
CCS feature What it tests IMG practice target Initial orders Recognition of instability and dangerous diagnoses Create emergency order bundles by presentation Time advancement Clinical judgment and monitoring Advance only after stabilizing and placing key orders Reassessment Response to treatment Check vitals, symptoms, focused exam, and new results Disposition Safe level of care Practice admission, ICU, discharge, and follow-up decisions Closure counseling Prevention and communication Add focused counseling only after acute management is safe Use a universal case framework, then adapt it by presentation
SODA framework for CCS
Stop treating CCS like a memorized order list.
Correct orders still need the right order.
Build high-yield order sets without becoming a checklist robot
Presentation Immediate danger Orders to rehearse Common trap Chest pain ACS, dissection, PE, pneumothorax ECG, troponin, monitor, aspirin when appropriate Waiting for labs before ECG Dyspnea Hypoxemia, asthma, CHF, PE, pneumonia Pulse ox, oxygen if low, CXR, ECG, targeted therapy Giving oxygen to everyone without indication Fever and hypotension Sepsis or shock Cultures, lactate, antibiotics, fluids, source workup Delaying antibiotics for complete results Focal weakness Stroke, bleed, hypoglycemia Glucose, neuro exam, head imaging, stroke pathway Skipping glucose or swallow safety Office prevention Missed chronic risk Screening, vaccines, adherence, follow-up Using emergency orders in a stable office visit Avoid IMG-specific mistakes that lower CCS performance
Red flag CCS behaviors
Safe CCS behaviors
A four-week CCS practice plan for IMGs
Week Main goal Daily task Review metric 1 Interface and emergency scripts 2 to 4 cases plus first-order rehearsal Could you stabilize before diagnosing? 2 Outpatient and prevention Mixed office and chronic disease cases Did closure include follow-up and counseling? 3 Timed mixed execution Timed random cases with no category preview Which miss type repeated? 4 Fatigue-proof performance Cases after MCQs or work shift Did your sequence stay safe under pressure? How to review a CCS case after you finish it
Case review template
Rapid-review checklist for exam day
Before advancing time
After results return
Before case closure
References
CCS Cases
Step 3 CCS Cases for IMGs: The Complete Practice Guide

For CCS timing and order logic
CCS is not just what you order. It is when you order, reassess, and close the case.
MDSteps helps you practice live CCS cases with vitals, orders, labs, time advancement, reassessment, closure, and after-action feedback.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.
Live case flow
Practice vitals, orders, labs, consults, treatments, and reassessment as the patient changes.
Order timing
Learn what must happen now, what can wait, and what loses value when late.
After-action feedback
See missed, late, unsafe, and unnecessary actions after each case.
IMG high-yield principle: treat the CCS screen as a simulated clinical shift. Every minute should either improve safety, clarify diagnosis, reassess response, or prepare a safe disposition.
Stabilize: address airway, breathing, circulation, mental status, pain, and unsafe location.
Order: place focused tests, monitoring, and treatments that fit the leading danger diagnoses.
Diagnose: interpret new data and remove diagnoses that no longer fit.
Act again: reassess, escalate, consult, discharge, counsel, or schedule follow-up.
CCS timing, orders, and reassessment
Free CCS demo cases
Live CCS case flowOrder timing reviewAfter-action feedback
Run free CCS demo cases first. Full access includes Step 3 QBank practice, CCS cases, analytics, and study planning.
CCS practice
Still missing the same kinds of questions?
Read why that happens.
Next step: practice with realistic cases, then compare your management against a structured miss log. For additional practice, visit MDSteps Step 3 and explore live CCS case practice.