Students scoring below 60% on Comprehensive Basic Science Self-Assessments usually do not need a larger pile of resources. They need a better diagnostic system. Pathology sits at the center of that system because Step 1 questions often test disease mechanisms through organ-system reasoning, not isolated memorization. A low score is rarely caused by one weak fact bank. It is more often caused by incomplete illness scripts, unstable basic science links, and passive review that does not force recall under exam conditions. The best Step 1 pathology review for low NBME scores starts with a simple question: when you miss a pathology question, what actually failed? The answer is usually one of five categories. You may not recognize the diagnosis from the vignette. You may recognize the disease but forget the mechanism. You may know the mechanism but miss the histology, gross pathology, or lab pattern. You may confuse two similar diseases. Or you may understand the disease but choose a distractor because the question asks for the next mechanistic link rather than the label. For a student below 60%, the goal is not to become a pathology encyclopedist. The goal is to build reliable recognition pathways. A board-style item often begins with age, timeline, risk factor, or exposure. It then adds a symptom cluster and a lab, imaging, or microscopic clue. The final question stem asks for pathogenesis, complication, diagnosis, or treatment principle. If your review only rereads textbook paragraphs, you may feel familiar with the topic but still fail to execute this sequence. Core principle: every pathology topic should be converted into a three-part script: trigger clues, mechanism, and tested consequence. If one part is missing, the script will collapse during an NBME block. Students below 60% also tend to overvalue rare details and undervalue common disease frameworks. For Step 1, hypertrophic cardiomyopathy is not only a memorized association with sudden death. It is a pattern of sarcomere mutation, asymmetric septal hypertrophy, dynamic outflow obstruction, systolic murmur behavior, and myocyte disarray. Minimal change disease is not only nephrotic syndrome in a child. It is selective albuminuria, podocyte foot process effacement, T-cell mediated cytokine injury, and steroid responsiveness. These frameworks help you answer new questions, not just repeated ones. Use NBME performance reports as a map, not a verdict. The NBME self-assessment ecosystem is designed to help examinees gauge readiness, and Step 1 content is organized through integrated organ systems. That means a low score should guide targeted repair by system and process. Instead of saying, “I am bad at pathology,” translate the score into a repair order: renal immune injury, cardiovascular hemodynamics, pulmonary obstructive versus restrictive disease, endocrine neoplasia, neurodegeneration, and inflammation pathways. A practical recovery plan begins with one high-yield pathology pass, one question-driven application pass, and one mixed-block readiness pass. The first pass fixes the map. The second pass tests whether the map works. The third pass tests whether you can retrieve it when the organ system is not announced. This is the difference between knowing pathology and passing Step 1 with pathology. The fastest way to improve from below 60% is to stop treating every missed question equally. A student who misses Wegener granulomatosis because they forgot c-ANCA needs a different intervention than a student who knew c-ANCA but failed to connect chronic sinusitis, hemoptysis, and rapidly progressive glomerulonephritis. Both questions are “wrong,” but the learning prescription is different. Your error log should identify the failure mode. Create five columns: organ system, disease process, missed clue, failed link, and repair action. The repair action must be concrete. “Review vasculitis” is too broad. “Compare granulomatosis with polyangiitis, microscopic polyangiitis, and eosinophilic granulomatosis with polyangiitis using vessel size, ANCA pattern, lung findings, kidney findings, and asthma association” is useful. The goal is to make your next study session obvious. Below 60%, do not write long explanations into your log. Long notes often become a second textbook that you never review. Keep each entry short enough to become a flashcard, a comparison table, or a five-minute whiteboard drill. The strongest entries are written as testable prompts. For example: “Adult with hemoptysis plus hematuria: what immune injury patterns separate anti-GBM disease from ANCA-associated vasculitis?” This format trains the exact retrieval process Step 1 requires. You should also classify misses as content gaps or reasoning gaps. A content gap means you lacked a fact needed to solve the question. A reasoning gap means the fact was present somewhere in your memory, but you did not apply it. Low NBME scores often contain both, but the ratio matters. If most misses are content gaps, you need a structured organ-system pathology pass. If most are reasoning gaps, you need more mixed questions, comparison drills, and explanation of why distractors are wrong. Use the error log to identify “NBME repeat themes.” These are concepts that appear across many diseases, such as necrosis patterns, granulomatous inflammation, oncogene versus tumor suppressor behavior, nephritic versus nephrotic syndromes, restrictive versus obstructive lung disease, shock physiology, and endocrine feedback loops. A low-scoring student can often gain more by mastering these cross-cutting frameworks than by memorizing rare pathology minutiae. MDSteps can support this process when used carefully. The Adaptive QBank includes more than 9000 questions, and missed questions can be converted into automatic flashcard decks that are exportable to Anki. Use those tools to make your error log active rather than decorative. The objective is not to collect mistakes. The objective is to make each mistake harder to repeat. When NBME scores are below 60%, many students try to reread every pathology chapter. This feels responsible, but it often wastes time because not every topic has equal value for your current score. Triage means ranking organ systems by three variables: frequency on your assessments, severity of weakness, and repairability. A weak but repairable system should receive priority over a broad system where your mistakes are scattered and inconsistent. Start by reviewing your last two NBMEs and your recent question blocks. Mark each missed pathology question by system. Then mark the mechanism family: inflammation, neoplasia, vascular injury, immunology, endocrine signaling, renal filtration, pulmonary mechanics, gastrointestinal injury, hematology, or neurologic degeneration. Patterns usually appear quickly. A student may think pathology is weak globally, but the real deficit may be renal, cardiovascular, and hematology. Another student may have broad recognition problems in every system because they never built disease scripts. The highest-yield triage order for many below-60% students is renal, cardiovascular, pulmonary, hematology-oncology, endocrine, gastrointestinal, neurologic, reproductive, musculoskeletal, and dermatology. This is not a universal ranking. It is a practical starting point because these systems contain dense mechanism chains and frequent distractor pairs. Renal questions often test immune injury, filtration barriers, acid-base logic, and nephritic versus nephrotic patterns. Cardiovascular questions test hemodynamics, congenital lesions, ischemia, cardiomyopathy, and vascular pathology. Pulmonary questions test mechanics, gas exchange, infection patterns, and tumor associations. List weak systems from NBME reports and recent timed blocks. Map each miss to a mechanism family, not only a diagnosis. Repair the two systems with the most repeated, fixable errors first. Within each system, review pathology in clusters. For renal, do not study diseases alphabetically. Study nephritic syndromes together, nephrotic syndromes together, tubular and interstitial disorders together, and renal vascular disorders together. For pulmonary, compare obstructive diseases, restrictive diseases, vascular disorders, infections, and neoplasms. For endocrine, link gland pathology to feedback loops. This organization mirrors how NBME distractors work. The wrong answer is often a disease that shares one clue but not the whole pattern. Each cluster should end with a closed-book recall drill. Example: “List the nephritic syndromes and write immune deposits, microscopy, complement pattern, and classic clue.” Then do 10 to 15 targeted questions. Do not wait until you feel ready. Questions reveal whether your framework is usable. After the block, update your table and create flashcards only for missed links. Use the official Step 1 content outline as a guardrail. Step 1 is integrated across organ systems, so pathology review should connect disease mechanisms to physiology, pharmacology, microbiology, and immunology. A cardiac ischemia question may test pathology, but the correct answer may depend on coronary anatomy or oxygen supply-demand balance. A pneumonia question may test inflammation, but the decisive clue may be an organism, host risk factor, or antibiotic mechanism. Isolated pathology review is only effective when it is integrated back into Step 1 reasoning. MDSteps turns practice-exam misses into targeted blocks, pivot-clue review, and miss-pattern tracking so the same NBME-style trap does not keep showing up. Pathology becomes testable when it is expressed as a chain. A weak chain looks like this: “COPD causes shortness of breath.” A Step 1 chain looks like this: chronic smoking causes airway inflammation, mucus hypersecretion, protease-mediated alveolar wall destruction, loss of elastic recoil, air trapping, increased compliance, and obstructive spirometry. The second version can answer questions about physiology, histology, symptoms, and complications. For each disease, write one mechanism chain that starts with the cause and ends with the finding. The chain should be short enough to say out loud. Good chains include a trigger, cellular injury, tissue change, physiologic consequence, and classic clue. For example, “anti-phospholipase A2 receptor antibodies injure podocytes, which disrupts the filtration barrier, causing heavy proteinuria, edema, and nephrotic syndrome in membranous nephropathy.” This format is stronger than a list of disconnected facts. When scoring below 60%, you should emphasize chains for common disease families: ischemic injury, coagulative necrosis, liquefactive necrosis, granulomatous inflammation, immune complex deposition, type II hypersensitivity, oncogene activation, tumor suppressor loss, metaplasia to dysplasia to carcinoma, and fibrosis after chronic injury. These families recur across organ systems. Once you understand them, many questions become variations rather than new material. Mechanism chains also protect you from distractors. Suppose a question describes a young patient with recurrent infections, absent thymic shadow, hypocalcemia, and conotruncal cardiac defect. If you only memorize “DiGeorge syndrome equals 22q11 deletion,” you may miss a question asking about failed development of the third and fourth pharyngeal pouches. If you know the chain, the answer follows. Pathology review should repeatedly ask, “What is upstream and what is downstream?” Use whiteboard retrieval for difficult chains. Close the resource, write the disease name, and reconstruct the pathway from memory. Then compare your answer to the source. The difference between what you wrote and what the source says is your true knowledge gap. This is more effective than highlighting because it exposes missing links. Evidence from learning science supports active retrieval and spaced practice as durable learning strategies, especially when learners must recall information rather than recognize it passively. Finally, attach each chain to a board-style clue. A chain without a clue may be scientifically correct but not exam-ready. For example, “berry aneurysm rupture causes subarachnoid hemorrhage” becomes testable when paired with sudden severe headache, blood in the subarachnoid space, and associations such as adult polycystic kidney disease. The practical unit of Step 1 pathology is not a paragraph. It is a clue-linked mechanism. Below 60%, question practice should be structured, not random punishment. Your weekly plan should include targeted blocks to repair weak systems and mixed blocks to test retrieval under uncertainty. Targeted blocks build pattern recognition. Mixed blocks prevent false confidence. If you only do system-specific questions after reviewing that system, you may answer correctly because the topic is already announced. Step 1 does not announce the system before each item. Use a three-pass method. First, preview the disease framework for one organ-system cluster. Second, complete a targeted timed block of 10 to 20 questions. Third, review every missed or guessed item with a brief error-log entry. The next day, do five-minute retrieval drills from the same cluster before starting a different topic. Three to four days later, test the cluster again in mixed mode. This creates spacing, retrieval, and interleaving without turning the schedule into chaos. When reviewing questions, force yourself to explain why the correct answer is correct and why the best distractor is wrong. The distractor explanation is often where the score gain lives. If a stem describes nephrotic syndrome, the exam may test whether you can separate minimal change disease, focal segmental glomerulosclerosis, membranous nephropathy, diabetic nephropathy, and amyloidosis. The wrong choices are not random. They are nearby diagnoses with overlapping clues. Common trap: reading the explanation and thinking, “That makes sense,” is not the same as being able to retrieve the distinction on a new question. Convert every important distinction into a recall prompt. Timed practice matters. Many below-60% students have knowledge that is too slow. They can solve a question after three minutes but not in the time pressure of an exam block. Practice stems in phases. During content repair, allow careful thinking. During readiness training, enforce timing. A reasonable benchmark is to identify the diagnosis or mechanism family within the first 30 to 45 seconds for most pathology questions. If you cannot, your illness script needs repair. Use MDSteps analytics when your review becomes hard to interpret. A dashboard that separates performance by system and topic can prevent overreacting to one bad block. The automatic study plan generator can also help sequence weak areas so that pathology, physiology, and pharmacology are repaired together. Keep the tool subordinate to the method: diagnose the miss, repair the mechanism, retest with questions, and confirm with NBME-style performance. Do not reset a large QBank reflexively. A reset can hide your history and encourage repeated passive exposure. Instead, filter for incorrect and marked questions after each system repair. If you miss the same concept again, promote it to a high-priority flashcard or comparison table. If you now answer correctly with clear reasoning, retire it and move on. Efficient review is selective. The exam rewards accurate retrieval, not resource completion. A student below 60% needs a schedule that is aggressive but realistic. The plan below assumes that pathology is the major weakness and that the student has four weeks before a readiness decision. It can be compressed or extended, but the sequence should remain the same: triage, repair, mixed application, readiness confirmation. Do not spend the first two weeks only watching videos. Every day should include retrieval and questions. Each day should begin with retrieval before input. Spend 15 minutes writing yesterday’s mechanisms from memory. Then check your work. This short drill tells you whether learning survived overnight. Next, complete your main system task. For example, a renal day might include nephritic versus nephrotic patterns, then a targeted renal pathology block, then review of misses. End with a mixed mini-block or a flashcard session from older misses. Use protected time for the highest-yield systems. If you have four study hours, do not split them into eight shallow tasks. Use two hours for one major system, one hour for questions, and one hour for review and flashcards. If you have a full day, use two system blocks and one mixed block. The key is finishing each topic with a testable output: a table, a mechanism chain, a flashcard set, or a corrected missed-question explanation. NBME checkpoints should not be taken too frequently. A self-assessment is useful when it changes your decision-making. If you take one every few days, you may burn through exams before you have repaired the cause of the low score. A practical rhythm is to take an NBME after a meaningful repair period, then spend one to two days reviewing it deeply. The review should identify repeated pathology mechanisms, not only count mistakes. Protect sleep and recovery. Pathology requires integration. Exhausted students often confuse similar diseases and overlook negative clues. If your schedule produces worsening focus and careless reading, it is not disciplined. It is counterproductive. Use shorter, higher-quality blocks with immediate review. The student who reviews 40 questions carefully usually gains more than the student who completes 120 questions with superficial explanations. Several pathology traps repeatedly hold students below 60%. The first is mistaking recognition for mastery. You may recognize a term such as “caseating granuloma” but fail to connect it to type IV hypersensitivity, macrophage activation, tuberculosis, fungal infections, or the differential with noncaseating granulomas. Recognition feels fluent. Retrieval proves mastery. The second trap is studying diseases without contrasts. Step 1 frequently tests boundaries. Ulcerative colitis and Crohn disease share chronic inflammatory bowel disease, but they differ by distribution, depth, complications, granulomas, fistulas, and cancer risk. Hodgkin lymphoma and non-Hodgkin lymphoma differ by spread pattern, Reed-Sternberg cells, extranodal involvement, and associations. Nephritic and nephrotic syndromes differ by inflammation versus permeability, hematuria versus heavy proteinuria, and RBC casts versus lipiduria. Review should emphasize these boundaries. The third trap is overfocusing on pathology while ignoring linked physiology. A restrictive lung disease question may require lung volumes. A valve lesion question may require pressure-volume loops. A renal tubular disorder may require acid-base logic. Pathology is the lesion, but Step 1 often asks for the functional result. When reviewing a disease, always ask, “What changes in physiology because of this lesion?” The fourth trap is treating histology as image memorization. Images are important, but they should be tied to mechanisms. A psammoma body should trigger papillary thyroid carcinoma, serous papillary ovarian carcinoma, meningioma, and mesothelioma, depending on the clinical setting. Auer rods should trigger acute myeloid leukemia and myeloperoxidase-positive blasts. Reed-Sternberg cells should trigger Hodgkin lymphoma and the appropriate subtype clues. The image is rarely enough by itself. The vignette decides the answer. The fifth trap is ignoring confidence. Record questions you guessed correctly. These are hidden weaknesses. A correct guess will not reliably repeat on a future NBME. Add guessed questions to your review queue if the reasoning was incomplete. You do not need to review every correct question in depth, but you should review every question where your confidence was low. Finally, avoid “resource switching” as an emotional response to a bad score. A new pathology resource may help if it solves a defined problem. It will not help if the real issue is passive review, weak error analysis, or poor mixed-block timing. Before switching, ask what the new resource will do that your current method does not. If the answer is unclear, fix the method first. In the final stage, pathology review should become lighter, faster, and more integrated. You are no longer trying to relearn every disease. You are stabilizing the patterns most likely to affect your exam. Use your error log to select 20 to 40 high-risk concepts. These should include repeated misses, guessed corrects, and topics that create confusion across systems. Convert each into a rapid prompt. Your readiness decision should be based on trend, not hope. A single improved block is encouraging, but NBME-style performance matters more. Review whether your errors are decreasing in the systems you targeted. Look for a change in error quality. Early in recovery, misses may reflect failure to recognize common diseases. Later, misses should become narrower: a less common association, a second-order mechanism, or a detail you can repair quickly. That shift suggests progress. Do not take Step 1 while major pathology frameworks remain unstable. Red flags include repeated failure to identify common organ-system patterns, inability to explain missed questions after reading the explanation, severe timing problems in mixed blocks, and NBME performance that remains below your school or advisor’s safe threshold. In those cases, more time should be used for targeted repair, not broad rereading. When you are approaching the exam, reduce new content and increase retrieval. Use short tables, flashcards from missed questions, and timed mixed blocks. The final week is not the time to discover a completely new pathology resource. It is the time to prove that your existing frameworks can be recalled quickly and accurately. A strong final review feels repetitive because the same high-yield patterns become automatic. For general Step 1 preparation support, review the MDSteps Step 1 resources. For clinical reasoning practice that connects clues to mechanisms, see the sample question breakdown. Use tools only when they improve the central workflow: identify the miss, repair the mechanism, retrieve it later, and retest it under exam conditions. Bottom line: low NBME pathology performance is fixable when you stop rereading passively and start repairing the exact links that fail under timed conditions. Build disease scripts, compare distractors, use spaced retrieval, and let your next NBME measure whether the repair worked. Medically reviewed by: Jonathan R. Feldman, MD, PhDWhy pathology drives recovery when NBME performance is below 60%
Build a diagnostic error log before adding another resource
Miss pattern
What it means
Repair action
Did not identify disease
Weak vignette pattern recognition
Create a clue stack: age, risk factor, symptom cluster, lab, histology
Identified disease but missed mechanism
Pathogenesis link is unstable
Write a one-sentence mechanism chain from trigger to finding
Confused similar diseases
Differential table is missing
Build a two-column contrast table and test it the next day
Changed correct answer
Poor confidence calibration
Record original reason, final reason, and the clue that should have decided it
Ran out of time
Recognition is too slow
Practice timed mixed blocks and cap review notes to three takeaways per miss
Use organ-system triage instead of rereading all pathology
Step 1
Step 2
Step 3
Do not just review your NBME misses. Re-test the pattern that caused them.
Understanding a miss is not the same as repairing it.
Turn pathology facts into mechanism chains
Framework
Ask yourself
Example Step 1 use
Cause to lesion
What injury creates the visible pathology?
HPV E6 and E7 alter tumor suppressor pathways in cervical neoplasia.
Lesion to physiology
How does the tissue change alter function?
Emphysema destroys alveolar septa and increases compliance.
Immune pattern
Which immune mechanism explains the labs?
Poststreptococcal glomerulonephritis follows immune complex deposition.
Timeline
Is the process acute, subacute, or chronic?
Coagulative necrosis evolves after myocardial infarction.
Practice pathology through questions, not passive completion
A four-week pathology rescue schedule
Week
Main objective
Daily work
Checkpoint
1
Diagnose weak systems and rebuild core mechanisms
Two organ-system clusters, 30 to 40 targeted questions, 30 minutes flashcards
Error log shows fewer repeated clue-recognition misses
2
Repair renal, cardiovascular, pulmonary, and heme-onc priorities
Mechanism chains, comparison tables, targeted blocks, short mixed set
Targeted blocks improve with correct reasoning, not recall alone
3
Move from system blocks to mixed pathology application
One mixed timed block, one focused repair block, spaced flashcards
Misses shift from major frameworks to smaller details
4
Confirm readiness and stabilize weak links
Mixed timed blocks, NBME review, rapid comparison drills
NBME performance supports a safe testing decision
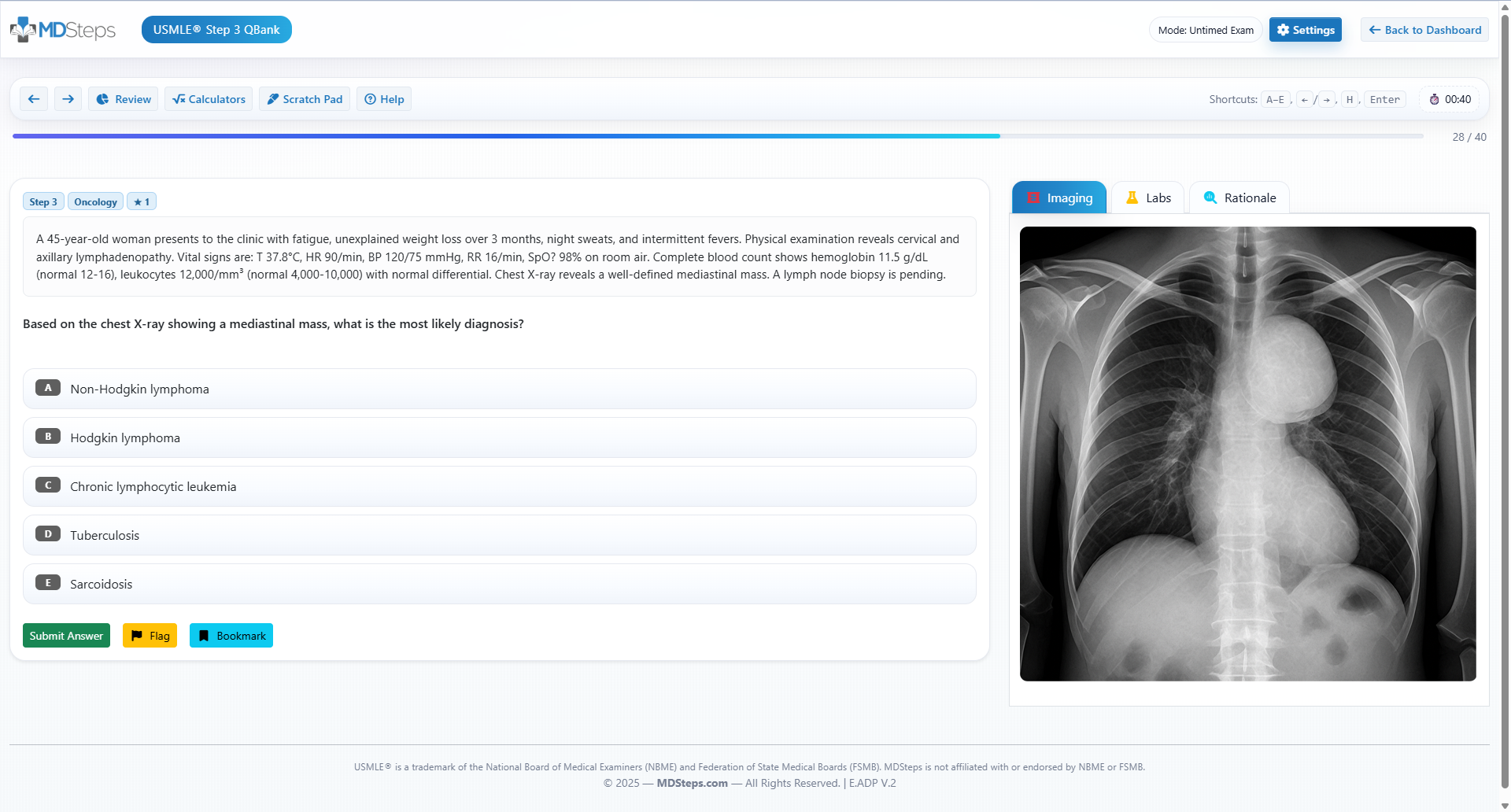
High-yield pathology traps that keep scores low
Rapid-review checklist and readiness decision
Rapid-review checklist
References
USMLE Step 1
Best Step 1 pathology review for students scoring below 60% on NBMEs
For NBME score plateaus and review
An NBME score report tells you what dropped. MDSteps helps show why it dropped.
Use MDSteps to sort NBME misses by weak system, reasoning trap, timing issue, distractor pattern, and readiness risk—then practice similar stems before your next assessment.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.
Practice-exam repair
Turn missed NBME concepts into targeted blocks instead of passive note review.
Pivot-clue review
Identify the clue that should have changed your answer before the choices pulled you away.
Readiness tracking
See which weak areas and miss patterns still need work before another assessment.
NBME score stuck?
Practice-exam repair loop
NBME-style practiceMiss-pattern reviewTargeted weak-area blocks
Start with a free reasoning review. Full access includes NBME-style blocks, analytics, flashcards, Step 3 CCS, and study planning.
After NBME review
Still missing the same kinds of questions?
Read why that happens.