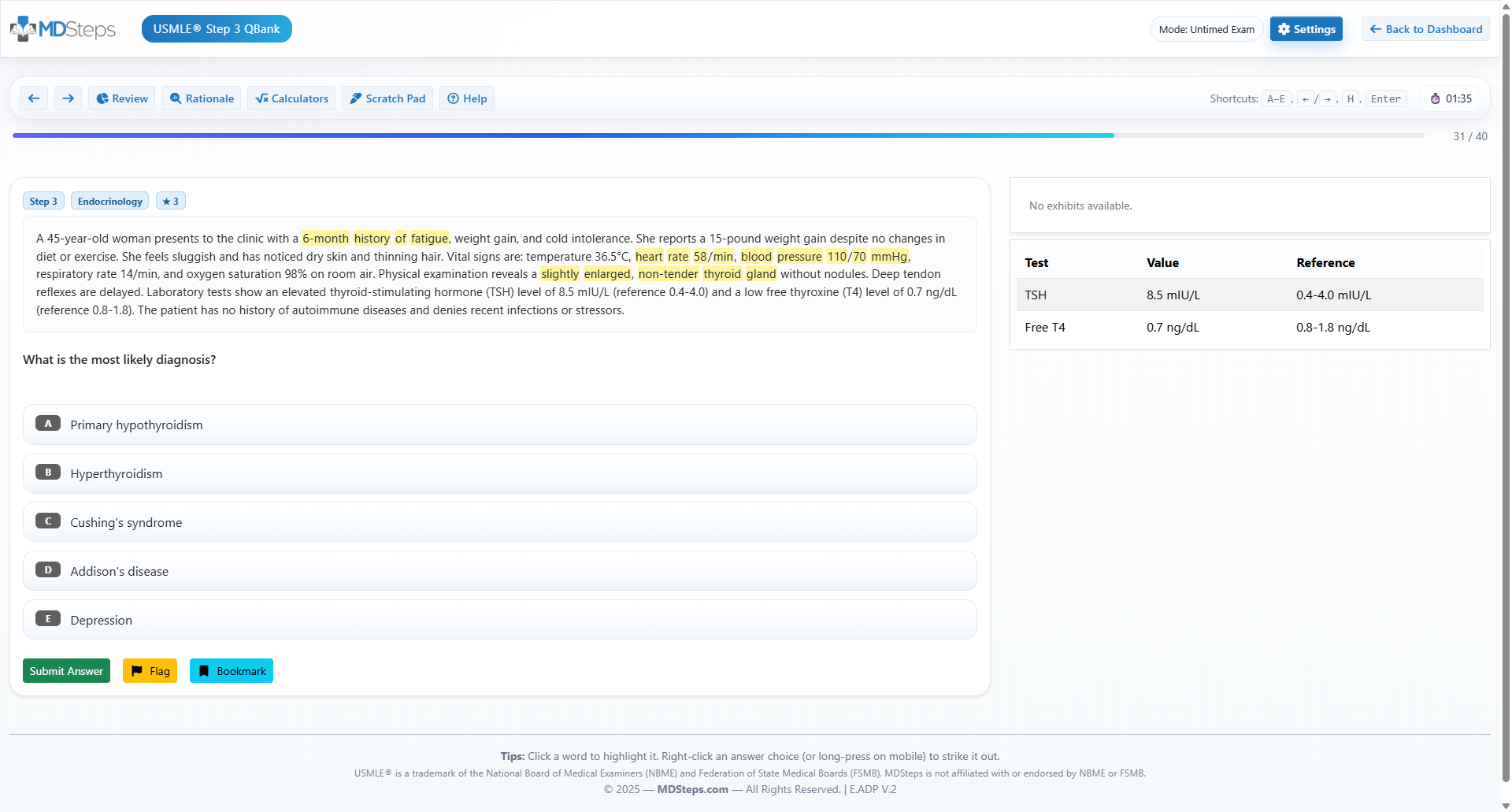
A failed CBSE should not be treated as a verdict on your ability to pass Step 1. It is a diagnostic signal. This guide turns that signal into a structured, exam-focused recovery plan. The most useful response to a failed CBSE is not panic, a new stack of resources, or a calendar packed with passive review. The correct response is diagnosis. The Comprehensive Basic Science Examination is designed as an integrated assessment of basic science knowledge and Step 1 readiness. It samples the same broad domain that matters for USMLE Step 1: mechanisms of health, disease, pharmacotherapy, diagnosis, communication, and applied foundational science. Because of that overlap, a low score often tells you where your Step 1 preparation system is breaking. A strong Step 1 study plan after failed CBSE begins with separating three problems that students often blend together. The first is knowledge deficit. This means the student truly does not know a concept, such as the pathophysiology of nephritic syndromes, mechanisms of antiarrhythmics, or enzyme defects in glycogen storage disease. The second is recognition deficit. Here, the student studied the content but fails to identify it in a clinical vignette. The third is execution deficit. This student reaches the right concept but loses points through timing, second-guessing, distractor attraction, or poor use of laboratory clues. CBSE remediation works when each missed question is assigned to one of those categories. Students who only reread First Aid after every miss may improve slowly because rereading treats all errors as knowledge errors. Board questions do not reward familiarity. They reward retrieval, discrimination, and application under time pressure. A student who misses hyperkalemia physiology because they forgot the effect of aldosterone needs content repair. A student who knows aldosterone but misses primary adrenal insufficiency because they overfocused on skin hyperpigmentation needs clue weighting. A student who changed the correct answer needs decision discipline. Before rebuilding the schedule, obtain the score report, list weak organ systems, and record performance by task if available. Prioritize systems that combine high frequency with low confidence. A low score in cardiovascular, renal, endocrine, immunology, microbiology, and pathology usually deserves earlier attention than an isolated weakness in a smaller domain. The goal is not equal time for every subject. The goal is maximal score movement per study hour. You could not explain the tested mechanism before seeing the answer explanation. You knew the topic but missed the vignette pattern or key clue. You reached the right concept but lost the question through timing or answer changes. Do not define readiness by mood. Students often feel worse as they study better because they finally see the size of the task. Define readiness by objective markers: rising NBME or CBSSA performance, fewer repeated misses, better timing, stronger mixed-block accuracy, and a stable passing probability close to the exam window. The failed CBSE becomes useful only when it leads to measurable changes in the way you study. Most students who fail CBSE need structure more than intensity. Ten unfocused hours can produce less progress than five targeted hours with active retrieval, question review, and spaced repetition. A practical recovery plan should have three phases: stabilization, rebuilding, and exam simulation. The length can be adjusted, but the sequence should not be reversed. Students who jump directly into full mixed blocks without repairing major content gaps often keep repeating the same mistakes. The first two weeks should stabilize the highest-yield weak areas. This is not the time to reread an entire review book cover to cover. Use the CBSE report, prior question logs, and self-awareness to choose three to five major systems. For most students, this includes pathology, physiology, pharmacology, microbiology, immunology, and biochemistry pathways that repeatedly appear inside clinical vignettes. Each day should include a focused content block, targeted questions, and a short review of missed concepts. Weeks three and four should shift toward mixed practice. This transition is important because Step 1 rarely announces the topic. A vignette may begin with anemia but test renal physiology. It may appear to be pharmacology but require autonomic receptor logic. Mixed blocks train the mind to identify the task before selecting the fact. During this phase, missed questions should be reviewed for mechanism and for the exact clue that should have redirected your thinking. Weeks five and six should emphasize readiness confirmation. Use timed mixed blocks, NBME-style self-assessments, and practice with break strategy. The goal is not to memorize more facts every day. The goal is to prove that your knowledge can survive exam conditions. If scores remain unstable, delay the real exam when possible and continue targeted remediation. Step 1 is pass or fail, but the decision to sit should still be data-driven. A sample day should be simple. Start with 60 to 90 minutes of focused content repair on a weak system. Complete one timed block of questions related to that system early in the plan, then mixed later in the plan. Spend at least as much time reviewing the block as you spent taking it. Create or unsuspend only the flashcards that directly address missed mechanisms, not every sentence in an explanation. End the day with 30 to 45 minutes of spaced repetition and a short list of the next day’s targets. After a failed CBSE, many students feel tempted to retreat into videos and notes because questions feel punishing. That instinct is understandable, but it slows recovery. Step 1 is a question-based exam, so questions must become the center of preparation. Content resources are tools for repairing specific gaps. They should not replace retrieval practice. The best question strategy depends on the phase of recovery. During the first phase, use targeted blocks to rebuild weak areas. A student with repeated endocrine misses should work through diabetes pharmacology, adrenal disorders, thyroid physiology, reproductive endocrinology, and related pathology in an organized sequence. Targeted work reduces cognitive overload and helps build a clean framework. Once performance improves, move to mixed blocks because real exam conditions require topic identification without warning. Review must be active. For each missed question, write a one-sentence takeaway in your own words. Then identify the decisive clue. A good entry is not “review nephrotic syndrome.” A useful entry is “heavy proteinuria, edema, hyperlipidemia, and fatty casts point to nephrotic syndrome; minimal change disease is associated with selective albumin loss and podocyte effacement.” The first entry is a vague task. The second is a retrievable exam pattern. Correct questions also deserve review, but not equally. If you answered correctly with uncertainty, treat it as a near miss. If you answered correctly because you eliminated poor options but could not explain the mechanism, repair the mechanism. If you answered correctly and can explain the concept quickly, move on. Efficient students do not review every word with the same intensity. They triage. The MDSteps Step 1 platform can support this process when used deliberately. Its Adaptive QBank with more than 9000 questions, automatic study plan generator, AI tutor, analytics dashboard, and flashcard decks from missed questions are most useful when they are tied to a daily error log. The platform should not be used as another passive content library. It should be used to expose weak patterns, force retrieval, and convert misses into spaced review. Students should also avoid the trap of measuring progress by the number of questions completed. Volume matters, but only after review quality is preserved. Completing 120 questions per day with superficial review may create the illusion of progress while leaving the same errors intact. A student recovering from CBSE failure often benefits more from 40 to 80 well-reviewed questions daily than from rushed high-volume blocks. If you keep narrowing stems to two answers and picking the distractor, the problem may not be your medical knowledge. MDSteps shows the pivot clue, the trap answer, and the reasoning pattern behind the miss—then turns it into targeted practice. A failed CBSE does not mean every system is equally weak. Starting over from page one wastes time and reduces confidence. Instead, repair systems in layers. The first layer is core physiology. The second is pathology patterns. The third is pharmacology and microbiology integration. The fourth is vignette discrimination. This sequence matters because Step 1 questions often test a mechanism hidden inside a clinical presentation. For cardiovascular topics, begin with pressure-volume loops, murmurs, shock physiology, congenital lesions, autonomic drugs, and antiarrhythmics. For renal topics, prioritize acid-base disorders, nephritic and nephrotic patterns, diuretics, tubular defects, and renal endocrine functions. For endocrine, focus on thyroid states, adrenal disorders, diabetes drugs, calcium regulation, and reproductive endocrine feedback. For immunology, master hypersensitivity reactions, immunodeficiencies, transplant concepts, and cytokine patterns. For microbiology, shift from organism lists to clinical syndromes, virulence factors, toxins, and drug mechanisms. Biochemistry deserves special handling. Many students try to memorize pathways in isolation and then miss the vignette because the exam asks for the consequence of enzyme failure, not the pathway diagram. Study biochemistry by clinical trigger. A child with fasting hypoglycemia, hepatomegaly, and lactic acidosis should immediately trigger glycogen storage disease logic. A patient with lens dislocation and thrombosis should trigger homocystinuria. A newborn with vomiting after feeding should trigger urea cycle, organic acidemia, or galactosemia patterns depending on associated clues. Pharmacology should be organized by mechanism, adverse effect, and contraindication. Step 1 rarely asks whether you have seen a drug name. It asks whether you understand receptor action, pathway blockade, toxicity, or resistance. The same principle applies to microbiology. Do not memorize organisms only by taxonomy. Organize by presentation, such as pneumonia in a patient with alcoholism, meningitis in a neonate, diarrhea after antibiotics, or painless genital ulcer. When reviewing a weak system, make a two-column list: “must know cold” and “recognize if seen.” Must-know topics include mechanisms repeatedly tested across questions. Recognize-if-seen topics include lower-frequency details that can be reviewed briefly but should not dominate the schedule. This distinction protects time and prevents perfectionism. The goal of system repair is not to feel complete. The goal is to reach the point where mixed questions become learnable rather than chaotic. Once you can explain the main mechanisms in a system and answer targeted questions with improving accuracy, return to mixed practice. Students who fail CBSE often respond in one of two ineffective ways. Some take too many practice exams too early and become discouraged by repeated low scores. Others avoid assessments until the end and discover too late that their plan did not work. The better approach is scheduled assessment with a clear purpose. A baseline assessment is useful only if it changes the plan. After CBSE failure, the school-administered score often already serves as a baseline. The next NBME-style exam should usually occur after a meaningful block of remediation, not two days later. Taking another exam before changing the study process mostly measures the same weakness again. A reasonable rhythm is one major self-assessment every 10 to 14 days during recovery, with more frequent timed QBank blocks between them. When reviewing an assessment, avoid obsessing over single-question memory. Instead, group misses by concept. If five misses involve renal physiology but appear as different diagnoses, the issue is not five separate facts. It is one unstable framework. If repeated misses involve communication or ethics, do not dismiss them as “soft” points. Step 1 includes communication and interpersonal skills, and these questions can be earned with structured practice. Readiness should be judged by trend, not one score. A single good score can occur from favorable content distribution. A single poor score can occur from fatigue, anxiety, or an unusually weak form. A stable upward pattern across timed mixed blocks and NBME-style assessments is more persuasive. Students should also consider testing conditions. A practice score taken untimed, with long breaks, or after reviewing similar topics may overestimate readiness. CBSSA can be especially helpful near the end because it provides an estimated probability of passing Step 1 if testing within one week. That probability should not be interpreted as a guarantee. It is a decision aid. If the estimate remains marginal, the plan should continue. If it is consistently reassuring across more than one data point and daily performance supports it, the student can approach the exam with more confidence. Assessment review should produce a short action list, not a new identity. Write down the top three content areas, the top two reasoning errors, and one execution habit to fix. Then revise the next week’s schedule around those items. This is how self-assessments become instruction rather than judgment. Many students who fail CBSE are not simply underprepared. They are also inefficient under pressure. Step 1 requires sustained attention across long timed blocks. A student may know enough to pass but still lose points through slow reading, overmarking, excessive answer changes, and mental fatigue. These are trainable skills. Timing should be practiced before the final week. Start with timed tutor-off blocks, even when reviewing a weak area. If timing is very poor, begin with smaller timed sets and build toward full blocks. Track not only percent correct but also questions left at the end, marked questions, and changes from correct to incorrect. A high number of marked questions often means the student lacks a decision threshold. Mark only questions that require return. Do not mark every uncomfortable question. A useful Step 1 decision rule is: identify the task, choose the best-supported answer, and move unless a specific clue contradicts it. Many wrong answer changes happen because the student replaces evidence with anxiety. If you change an answer, you should be able to name the new clue that makes the original answer wrong. A vague feeling is not enough. Stamina improves through simulation. During the final phase of recovery, complete multiple timed blocks with planned breaks. Practice food, hydration, and screen endurance. Do not discover on exam day that caffeine causes tremor, that heavy meals cause fatigue, or that you cannot sustain attention after three blocks. These details matter because Step 1 performance is not only knowledge. It is knowledge delivered under standardized conditions. Students should also build a reset routine. After a difficult question, take one breath, release the previous item, and start the next vignette clean. Carryover frustration is a silent score killer. One missed question should not become five. Change an answer only when you identify a concrete clue that makes your first choice inconsistent with the stem. Anxiety alone is not evidence. Execution training is especially important for students whose QBank review shows many near misses. If you frequently narrow choices to two and choose the wrong one, focus on contrast tables. Write why the correct answer is better and why the tempting distractor is wrong. Step 1 often tests distinctions: nephritic versus nephrotic syndrome, SIADH versus cerebral salt wasting, acute intermittent porphyria versus lead poisoning, or type I versus type IV hypersensitivity. Mastering these contrasts produces large gains. The first mistake is resource switching. A failed CBSE can make every new resource look like the missing solution. In reality, most major Step 1 resources can work if used actively. Constant switching creates shallow exposure without consolidation. Choose one primary QBank, one concise content reference, one spaced repetition system, and one assessment plan. Add resources only when they solve a specific problem. The second mistake is treating Anki as a substitute for question reasoning. Flashcards are powerful for spaced retrieval, but Step 1 requires context. A card may help you remember that osteoclasts are activated by RANKL, but a vignette may test the consequence of denosumab or the mechanism of osteoporosis. Use flashcards to stabilize facts and mechanisms. Use questions to learn application. The third mistake is reviewing explanations passively. Reading a beautiful explanation is not the same as being able to answer the next question. Convert explanations into retrieval prompts. Ask: what was the diagnosis, what clue proved it, what mechanism was tested, what answer did I choose, and why was that option wrong? The fourth mistake is ignoring wellness until burnout appears. CBSE failure can be emotionally heavy, especially when school progression or exam eligibility depends on it. Students should protect sleep, movement, meals, and at least brief social support. This is not motivational advice. Sleep and attention directly affect memory consolidation and timed performance. A plan that requires chronic exhaustion is not a serious plan. The fifth mistake is using raw QBank percentage as the only readiness marker. QBank percentages vary by resource, block composition, and whether questions are new or repeated. A rising trend is useful, but Step 1 readiness should include NBME-style performance, timing, stamina, and error stability. A student can have a respectable QBank percentage and still be weak on NBME-style integration. The sixth mistake is avoiding weak topics because they feel unpleasant. A recovery plan must attack the areas that cost points. Use shorter sessions for difficult subjects if needed, but do not skip them. Confidence grows from repeated contact with previously weak material. MDSteps can be helpful here when used as a control system rather than another distraction. The analytics and exam readiness dashboard can show whether weak domains are improving, while auto-generated flashcards from missed questions help prevent repeated losses. The value is not in doing more. It is in studying with feedback. In the final stretch, the plan should become narrower and more objective. The question is no longer “Do I know everything?” No student does. The question is whether you can consistently handle integrated Step 1 reasoning across timed blocks. The final checklist should include content, assessment, timing, and emotional control. For the last week, prioritize consolidation. Review your error log, high-yield contrasts, pharmacology mechanisms, microbiology syndromes, biostatistics formulas, ethics patterns, and repeatedly missed diagrams. Do not attempt to master a new comprehensive resource. New resources late in the process usually increase anxiety without improving retention. Students who failed CBSE can still pass Step 1, but the recovery must be honest. If your scores remain below a safe threshold, the better professional decision is to continue preparation. If your trend is stable, your timing is controlled, and recent assessments support readiness, trust the process you built. Step 1 rewards applied understanding, not perfection. For a focused next step, use a structured platform, a concise error log, and a realistic schedule. Students preparing for Step 1 can begin with the MDSteps Step 1 QBank and study tools, especially if they need adaptive practice, automatic missed-question flashcards, and readiness analytics in one workflow. Medically reviewed by: Daniel R. Moreno, MD, Internal Medicine.Treat the Failed CBSE as a Readiness Map
Knowledge deficit
Recognition deficit
Execution deficit
Build a Six-Week Remediation Calendar
Phase
Main objective
Daily work
Readiness marker
Weeks 1-2
Repair major content gaps
Focused system review, targeted questions, flashcards from misses
Fewer repeated misses in the same mechanism
Weeks 3-4
Convert knowledge into mixed-block recognition
Timed mixed QBank blocks, error log, short content patching
Rising mixed-block accuracy and better timing
Weeks 5-6
Confirm Step 1 readiness
NBME-style assessments, exam stamina practice, final weak-area review
Stable passing trend on recent assessments
Use Questions as the Primary Learning Engine
Missed Question Review Flow
Learn the patterns behind your misses. Break the plateau.
Still missing questions you thought you understood?
Repair Weak Systems Without Starting Over
Weak area
Repair focus
Common trap
Renal
Acid-base, diuretics, glomerular syndromes
Choosing diagnosis by one lab instead of the full pattern
Cardiology
Hemodynamics, murmurs, shock, autonomics
Memorizing sounds without understanding physiology
Microbiology
Syndromes, toxins, virulence, antimicrobials
Studying organism names without clinical context
Biochemistry
Clinical pathway consequences
Memorizing pathway order without vignette triggers
Use NBME-Style Assessments at the Right Time
Fix Timing, Stamina, and Decision Errors
Decision rule for answer changes
Avoid Common Recovery Mistakes
Rapid-Review Checklist Before Retaking CBSE or Sitting Step 1
References
USMLE Step 1
Best USMLE Step 1 study plan for students who failed CBSE
For students stuck despite doing more questions
UWorld explains the medicine. MDSteps explains the decision.
Traditional review often tells you the correct answer. MDSteps helps isolate the decision error: the missed pivot clue, the tempting distractor, the timing mistake, or the weak rule that failed under pressure.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.
Pivot-clue review
See the exact phrase in the stem that should have changed your decision.
Distractor trap logic
Learn why the answer you almost picked felt right—and why it was wrong for this patient right now.
Miss-pattern analytics
Turn repeated mistakes into targeted blocks, flashcards, and readiness signals.
Missed question
↓
Was the mechanism unknown?
↓ yes: repair content and make one card
Was the mechanism known but the vignette missed?
↓ yes: write the decisive clue and contrast with distractors
Was the answer changed or rushed?
↓ yes: add timing or decision rule to error log
Score stuck after more questions?
Free reasoning diagnostic
Pivot clue isolatedDistractor trap explainedNext study target identified
No credit card required for the free reasoning review. Full access is $27/month after that. Cancel anytime.
Reasoning diagnostic
Still missing the same kinds of questions?
Read why that happens.