Your Step 1 score usually stops improving when your review process is no longer changing your future answers. The problem may be a content gap, weak recall, timing pressure, or a repeated reasoning error like missing the pivot clue, falling for a distractor, or answering the wrong task. If your Step 1 NBME score is not improving, the most important first move is not adding more hours. It is diagnosing the failure mode. A stuck score usually means your current process is producing more exposure, but not more exam-ready retrieval. Students often respond by rereading notes, restarting videos, or buying another resource. Those actions feel productive because they increase contact with material. They do not necessarily improve the ability to solve a new NBME-style question under time pressure. Step 1 rewards integrated reasoning. A vignette may begin with a symptom, add a risk factor, show a laboratory clue, and ask for a mechanism, diagnosis, complication, or drug effect. The student must identify which detail changes the answer. A plateau develops when the study process trains recognition of familiar explanations, but the exam requires selection among close distractors. That is why a student may know the topic after reading the explanation and still miss the next question on the same concept. Do not treat every flat NBME score as the same problem. A score can be stuck because of weak content, poor question interpretation, inadequate recall, timing pressure, or an inefficient review loop. Each cause requires a different repair. Content weakness requires targeted rebuilding. Interpretation errors require question dissection. Recall problems require spaced retrieval. Timing problems require block pacing. Review problems require a system that converts each miss into a reusable rule. The first diagnostic question is whether your incorrect answers cluster by organ system, task, or question behavior. Organ system patterns include repeated misses in renal physiology, endocrine pharmacology, cardiopulmonary pathology, microbiology, or neuroanatomy. Task patterns include missing mechanism questions, next-step basic science applications, adverse effects, inherited disease patterns, or biostatistics interpretation. Behavior patterns include changing correct answers, ignoring a key lab, choosing a true but irrelevant statement, or rushing the final third of a block. Many students only review by topic. That is incomplete. Step 1 misses are often not caused by total ignorance of the topic. They are caused by failing to retrieve the right feature at the right moment. For example, a student may know that Kartagener syndrome involves primary ciliary dyskinesia, but miss the question because the vignette describes chronic sinusitis, bronchiectasis, infertility, and situs inversus without naming the syndrome. Another student may know the urea cycle, but miss the question because they cannot connect hyperammonemia after protein intake to the defective enzyme pattern. The problem is not just “biochemistry.” It is failure to translate a vignette into a mechanism. Begin with your last two NBME score reports and your most recent QBank blocks. Use them together. NBME forms estimate readiness and show broad performance patterns. QBank data reveals how you behave question by question. If the NBME score is flat but QBank percentage is rising, you may be memorizing the bank rather than improving transfer. If both are flat, your study method is likely not producing durable recall. If QBank timing is comfortable but NBME timing is stressful, your practice may not match exam pressure. A useful plateau diagnosis asks four questions. First, what content repeatedly appears in your misses? Second, what clue did you fail to use? Third, what wrong-answer trap did you choose? Fourth, what rule would help you answer the next version correctly? If your review does not answer all four, it will not reliably move the score. The goal is not to collect explanations. The goal is to convert errors into a smaller set of high-yield decision rules. For Step 1, the best rules are usually short and mechanism-based. “A patient with recurrent pyogenic infections and absent tonsils suggests X-linked agammaglobulinemia due to BTK mutation.” “A question asking which enzyme is inhibited by a statin is testing HMG-CoA reductase, not cholesterol absorption.” “A microcytic anemia with basophilic stippling and abdominal pain should trigger lead poisoning, not iron deficiency.” These rules are portable. They improve future questions because they connect clue, mechanism, and answer choice. Use the following diagnostic frame before changing resources. A resource change can help when the old resource is incomplete or poorly aligned. It can also hide the real problem by giving you new material to consume without fixing the reasoning error. The test is simple: if you cannot explain why you missed your last 30 questions using a stable taxonomy, the next resource will probably become another passive exposure source. A Step 1 score plateau often persists because students label every miss as a knowledge gap. This feels safe because the solution is familiar: read more, watch more, or annotate more. Yet many NBME misses occur when the student knew enough to answer correctly but failed to apply the information. Treating that as missing content creates a bloated study plan. It also prevents the student from repairing the actual test-taking process. Use a two-column diagnosis for every missed question: knowledge failure or reasoning failure. A knowledge failure means you did not possess the necessary fact, mechanism, association, or definition. You could not have answered correctly without learning something new. A reasoning failure means the necessary information was available in your memory or in the vignette, but you failed to use it. You selected a distractor, overweighted a familiar phrase, ignored the asked task, or answered a different question. This distinction matters because the repair is different. Knowledge failures need concise content rebuilding and retrieval. Reasoning failures need question reconstruction. For reasoning misses, reading the explanation twice is not enough. You must ask what made the wrong answer attractive and what clue should have stopped you. If the wrong answer was true but did not answer the stem, the issue is task control. If two answers seemed plausible, the issue is discriminating clue selection. If you picked a disease from one phrase while ignoring a conflicting lab, the issue is premature closure. The most useful review sentence begins with “I missed this because…” and ends with a change in future behavior. “I missed this because I did not know the drug adverse effect” is useful if it leads to retrieval. “I missed this because I saw diarrhea and chose VIPoma before checking potassium and acid-base status” is even more useful because it exposes a reasoning habit. It tells you what to stop doing. One common Step 1 trap is over-recognition. You see one familiar clue and jump to an answer before the vignette has finished building the diagnosis. For example, cough and fever may make pneumonia tempting, but the presence of recurrent infections, absent thymic shadow, or a specific immune-cell abnormality may shift the question toward immunodeficiency. A patient presents with episodic weakness after high-carbohydrate meals, but the question may not be asking for diagnosis. It may ask for the channel defect, inheritance pattern, or serum potassium change. The final task controls the answer. Another trap is topic-label review. Students write “missed renal” or “missed pharm” and move on. Those labels are too broad. “Renal” could mean Starling forces, nephritic versus nephrotic patterns, acid-base interpretation, diuretic physiology, or renal embryology. “Pharm” could mean mechanism, toxicity, contraindication, autonomic receptor effect, or antimicrobial spectrum. If your labels are broad, your repair will be broad. Broad repair produces slow score movement because it spends equal time on what you know and what you do not. Use a narrower taxonomy. For every miss, tag the organ system, discipline, task, and error behavior. A useful entry might read: “Cardiovascular, physiology, mechanism, ignored preload clue.” Another might read: “Microbiology, pharmacology, treatment mechanism, confused folate synthesis inhibitors.” After 40 to 60 entries, the pattern becomes visible. You may discover that your “content problem” is really an autonomic pharmacology discrimination problem, or that your “timing problem” is actually excessive rereading caused by weak task anchoring. Once the pattern is visible, your study plan becomes smaller and sharper. That is the point. A plateau does not require studying everything harder. It requires studying the repeated failure points more deliberately. The student who fixes five recurring reasoning errors can gain more than the student who passively rereads five chapters. Approach your NBME score report as a clinical data set. A physician does not treat a fever by saying “the patient is sick” and ordering everything. The physician localizes the problem, interprets the pattern, and selects the next test or treatment. A Step 1 plateau should be handled the same way. The score is the vital sign. The missed-question pattern is the history, examination, and laboratory data. Begin with three NBMEs if available. One exam can reflect variance. Two exams show direction. Three exams show a pattern. If you only have one official self-assessment, combine it with your most recent timed mixed QBank blocks. Do not compare a tutor-mode block on a single subject with an NBME form. That is not an equal comparison. Mixed timed conditions reveal whether you can retrieve information when the topic is not announced. For each NBME, record total performance, system performance, discipline performance, and the categories that felt hardest during the exam. Feeling matters less than data, but it can reveal cognitive load. If every long physiology stem feels slow, that suggests a process problem even before you count misses. If every microbiology question feels binary, that may suggest memorization without discriminators. If every biostatistics item feels unfamiliar, that is likely a focused content gap. Compare recent NBMEs under similar conditions. Look for a true plateau, not one low test. Sort misses by system, discipline, task type, and behavior during the question. Decide whether the miss was content, mechanism, distractor, task, timing, or recall. Assign a targeted repair and retest the same skill within the same week. When reviewing a score report, avoid two misleading conclusions. First, do not assume your lowest system is always your highest priority. A low category with few questions may be less important than a moderate deficit in a heavily tested area. Second, do not assume your highest system is safe. High performance can hide subtopic gaps. A student may perform well in cardiovascular overall while repeatedly missing murmurs, pressure-volume loops, or antiarrhythmic mechanisms. Use weighted decision-making. Prioritize topics that are weak, frequent, and fixable. Weak means your performance is below your target. Frequent means the topic appears often enough to affect readiness. Fixable means you can improve it with a defined intervention. For example, endocrine feedback loops are usually fixable because the same principles recur. Random rare facts may be less efficient unless they are repeatedly appearing in your misses. Next, identify whether your plateau is horizontal or uneven. A horizontal plateau means many subjects are mildly weak. This often happens when students have incomplete foundations or too much passive review. The repair is a balanced weekly cycle of mixed questions, targeted content, and spaced retrieval. An uneven plateau means one or two domains repeatedly drag down performance. This requires a focused sprint. A student who repeatedly misses renal physiology should not spend equal time on dermatology minutiae. Do not ignore correct answers. Review a sample of correct questions, especially those guessed between two options. Correct guesses may conceal unstable reasoning. Mark them as “fragile correct.” If you got the answer right but cannot explain why the wrong answer was wrong, the concept is not secure. Fragile corrects often become incorrect on the next NBME because the new form changes the surface details. Use a three-pass audit. On pass one, list missed topics without reading full explanations. On pass two, read explanations and classify the error. On pass three, write the future rule. This protects you from explanation fluency. Explanation fluency occurs when the answer feels obvious after the resource explains it. That feeling is not the same as independent retrieval. The question to ask is, “Could I have generated this answer before seeing the explanation?” After the audit, build a one-page diagnosis. Include your top three content deficits, top three reasoning errors, top two timing problems, and top two review weaknesses. Then create a weekly plan that targets those items. If the plan is not tied to the audit, it is not a diagnosis-driven plan. It is a hope-driven plan. Students often ask when to take the next NBME. The answer depends on whether you have changed the process. Taking another form without repairing the pattern mostly measures the same problem again. Use a new form after you have completed a focused repair cycle and tested the repaired skills in mixed timed blocks. The purpose of the next NBME is to validate the intervention, not to provide emotional reassurance. MDSteps turns practice-exam misses into targeted blocks, pivot-clue review, and miss-pattern tracking so the same NBME-style trap does not keep showing up. The review loop is the engine of score improvement. If the loop is weak, more questions produce more exposure but not more growth. A strong loop has four parts: attempt, diagnose, encode, and retest. Most plateaued students complete only the first two. They attempt questions and read explanations. They do not encode a rule, and they do not retest that rule soon enough to make it durable. A good review loop starts before the explanation. After choosing an answer, briefly state your reasoning. You can do this mentally or in a short note. Write what clue you used and why you eliminated the closest distractor. This creates a record of your thought process. Without it, the explanation can overwrite your memory of why you missed the question. You may think, “I just forgot that fact,” when the real problem was that you misread the final sentence. After the explanation, reduce the miss to a transferable rule. Avoid copying paragraphs. A rule should be short enough to review during a later session. It should include a trigger, a concept, and an action. For example: “Painless hematuria with red cell casts points to glomerulonephritis, not lower urinary tract bleeding.” “A competitive antagonist shifts the dose-response curve right without lowering maximal effect.” “A question asking for the cause of edema in nephrotic syndrome is testing urinary protein loss and reduced plasma oncotic pressure.” Then decide where the rule belongs. Content rules belong in a spaced flashcard deck or active recall sheet. Reasoning rules belong in a test-day rule list. Timing rules belong in your block strategy. Do not mix everything into one giant notebook. Large notebooks often become archives rather than tools. The best system is small, retrievable, and revisited. The retest step is where many students lose points. If you write a rule but never retrieve it, it remains inert. Retest within 24 to 72 hours using a related question, a self-generated vignette, or a flashcard that forces application. Recognition is not enough. A card that asks “What is the mutation in Marfan syndrome?” tests recall of a fact. A better applied prompt asks, “Tall patient with lens dislocation, aortic root dilation, and long extremities. What protein is defective and what signaling pathway is affected?” The second prompt resembles Step 1 reasoning more closely. For mechanism-heavy content, use why-chains. A why-chain links the vignette to the answer in three to five steps. For example: chronic kidney disease causes decreased erythropoietin, which reduces red blood cell production, which causes normocytic anemia. Another example: cystic fibrosis causes defective chloride transport, which thickens secretions, which causes recurrent respiratory infections and pancreatic insufficiency. Why-chains train causality. Step 1 often tests causality. For pharmacology, separate four tasks: mechanism, use, adverse effect, and contraindication. Many students review drugs as if knowing one task covers all tasks. It does not. A question may describe a drug by its receptor effect, ask for toxicity, or ask which patient should not receive it. A stable review loop forces you to identify which drug task you missed. “Beta-blocker” is too broad. “Nonselective beta-blocker may worsen asthma by blocking beta-2 mediated bronchodilation” is a usable rule. For pathology, connect gross findings, microscopy, and mechanism. Step 1 often shifts between these representations. You may get the same disease as a biopsy description, a lab pattern, a pathophysiologic mechanism, or a complication. A student who only memorizes the name may fail when the representation changes. During review, ask, “How else could this concept appear?” That question builds transfer. Use your QBank as a laboratory, not a scoreboard. A score on one block is less important than the quality of the review loop after it. Tutor mode can be useful for early learning, but plateau repair usually needs timed mixed blocks because they reveal retrieval failures. When you review, do not chase every detail with equal intensity. Prioritize details that explain the correct answer or eliminate a high-probability distractor. A strong loop also controls volume. Doing 120 questions poorly is less useful than doing 40 questions with precise repair. During a plateau, the goal is not maximum question count. The goal is maximum conversion of misses into future points. Once the loop becomes efficient, volume can increase without sacrificing learning quality. When NBME scores are stuck, students often increase passive re-exposure. They reread First Aid pages, replay videos, highlight explanations, or reorganize notes. These methods can clarify a topic, but they are weak tests of whether you can retrieve and apply information later. Step 1 is not a recognition exam. It is an applied recall exam under uncertainty. Your study method must therefore include deliberate retrieval. Active recall means producing the answer before seeing it. Spacing means returning to the concept after forgetting has begun. Together, they create durable learning. For Step 1, the practical form is simple: learn a concept, answer questions, make application-based recall prompts from misses, and revisit them over days. The goal is not to remember a page. The goal is to retrieve a mechanism when the vignette presents it in a new form. Passive review has a role. Use it when you truly lack the foundation to understand an explanation. If you cannot describe the renin-angiotensin-aldosterone system, you should rebuild it before drilling renal physiology questions. If you cannot explain T-cell maturation, immunodeficiency questions will feel random. But once the foundation exists, additional passive review has diminishing returns. The score moves when you repeatedly retrieve, apply, and correct. Make your recall prompts Step 1-shaped. A poor card asks, “What is the cause of Chediak-Higashi syndrome?” A stronger card says, “Child with recurrent pyogenic infections, partial albinism, peripheral neuropathy, and giant granules in neutrophils. What intracellular process is defective?” This prompt forces you to map clinical clues to lysosomal trafficking. It trains the same path the question requires. For students overwhelmed by flashcards, use a missed-question deck rather than a giant premade deck. Premade cards can be useful, but a plateau often needs personalization. Your missed-question deck should contain the concepts you failed to retrieve, not every possible fact. Limit each card to one decision. If a card tests three facts, you may answer one correctly and ignore the others. Clean cards expose weakness. Use a weekly spacing rhythm. Concepts missed today should be reviewed tomorrow, again in several days, and again the following week. The exact interval matters less than the principle: do not let a missed concept disappear until the next NBME. If a concept is repeatedly missed, promote it to a high-priority rule and test it through new questions. Repetition without variation can create memorization. Retrieval with variation creates transfer. Spacing also protects against a common plateau illusion. You may review a topic today and score well on questions immediately afterward. That does not prove readiness. Immediate performance can reflect short-term availability. Step 1 requires retrieval days or weeks later, while mixed with unrelated topics. To test readiness, answer related questions after a delay and without warning yourself which topic is coming. Interleaving helps for similar concepts. Study nephritic and nephrotic syndromes together after learning them separately. Compare restrictive and obstructive lung disease. Contrast primary adrenal insufficiency with secondary adrenal insufficiency. Compare congenital adrenal hyperplasia enzyme defects. Interleaving forces discrimination, which is exactly what NBME distractors require. Use memory tools carefully. Mnemonics help when the task is association. They are less useful when the task is mechanism. For example, a mnemonic may help remember lysosomal storage diseases, but you still need to know which accumulated substrate explains the presentation. Do not let a memory hook replace causal reasoning. The best Step 1 memory tools connect the hook to the mechanism. For students using MDSteps Step 1 resources, the most useful workflow is to let missed questions generate focused review, then convert those misses into automatic flashcard decks that can be exported to Anki. This keeps recall tied to actual errors rather than building a large generic deck that may not match your plateau. Step 1 questions often look like content questions, but the scoring difference comes from reasoning discipline. A student who knows many facts can still miss questions by failing to identify the task, overvaluing a distractor, or not translating a clinical clue into a mechanism. When your NBME score is stuck, question strategy should be rebuilt alongside content. Start each question by identifying the final task. Is the item asking for the diagnosis, mechanism, risk factor, pathologic finding, drug mechanism, adverse effect, inheritance pattern, or next experimental result? Many wrong answers are in the correct topic area but the wrong task category. If the stem asks for mechanism, a diagnosis answer may be tempting but irrelevant. If it asks for the most likely enzyme deficiency, a treatment choice is not the target. Next, identify the pivot clue. The pivot clue is the detail that changes the answer from a broad category to the specific correct choice. A patient presents with anemia and fatigue. That is broad. Add neurologic symptoms and hypersegmented neutrophils, and the path narrows toward vitamin B12 deficiency. Add a vegan diet, and the cause changes. Add ileal resection, and absorption becomes central. Add normal methylmalonic acid, and folate becomes more likely. The pivot clue controls the answer. When two answers feel correct, do not ask which one you like more. Ask which answer explains more of the vignette with fewer contradictions. Board-style questions are usually written so the correct answer accounts for the stem better than the distractor. A distractor may explain one clue but fail another. Train yourself to eliminate answers by contradiction, not by vague discomfort. Read the last sentence carefully. Name the category of answer before looking at choices. Find the specific detail that distinguishes the correct concept from the closest distractor. Ask why the tempting wrong answer is not fully supported by the stem. Use answer choices strategically. Before reading choices, predict the answer when possible. Prediction reduces distractor pull. If prediction is not possible, predict the category. For example, if the question asks for the mechanism of edema, decide whether the answer should involve hydrostatic pressure, oncotic pressure, lymphatic obstruction, sodium retention, or endothelial injury. Then read choices through that lens. For long stems, avoid drowning in details. Read the final sentence first if timing is tight. Then read the vignette with the task in mind. This does not mean ignoring the stem. It means organizing the stem. If the question asks for the organism, pay attention to exposures, immune status, stain, culture, and virulence factors. If it asks for pathophysiology, pay attention to the chain from presentation to mechanism. For experimental questions, slow down. These items often test the same content through graphs, cell models, receptor assays, or gene knockouts. Translate the experiment into a familiar pathway. Ask what was changed, what was measured, and what direction the result moved. Then connect the result to the mechanism. Students often miss these questions because the format feels unfamiliar, not because the concept is rare. For biostatistics and epidemiology, write down the structure. Do not rely on memory alone when a table is present. Identify true positives, false positives, false negatives, and true negatives. For study design questions, ask whether the investigators start with exposure, outcome, or a randomized intervention. The fastest way to improve these questions is to stop treating them as reading comprehension and start treating them as templates. For ethics and communication, choose the response that gathers information, acknowledges emotion, respects autonomy, and avoids premature reassurance. Step 1 communication questions often punish judgmental, dismissive, or overly directive language. The best answer usually keeps the clinical relationship open while addressing safety. If a patient presents with refusal, fear, or misunderstanding, first explore the concern unless there is an immediate safety emergency. Finally, rehearse your answer-changing rule. Change an answer only when you can name a specific clue you missed or a specific task error. Do not change because of anxiety. Many plateaued students lose points through late answer switching without evidence. A disciplined rule protects correct instincts while still allowing correction when a true misread occurs. Question strategy improves through deliberate practice. After each block, choose five questions that came down to two answers. For each, write why the wrong answer was tempting and what clue ruled it out. This exercise trains the exact discrimination that separates a stuck score from a rising score. A recovery plan should be short enough to execute and specific enough to change performance. When Step 1 NBME performance is stuck, a two-week diagnostic repair cycle is often more useful than a vague month-long plan. The purpose is to identify the highest-yield failure points, repair them, and retest under realistic conditions. The plan should not try to relearn all of medical school. It should target the repeated mechanisms that cost points. Start by selecting three priority domains. Use your audit, not your preferences. A domain can be an organ system, a discipline, or a reasoning skill. Examples include renal acid-base physiology, autonomic pharmacology, immunodeficiency patterns, microbe-drug matching, biostatistics tables, or mechanism questions with long stems. Each domain must have a defined output. “Study renal” is not an output. “Correctly interpret anion gap, respiratory compensation, and diuretic effects in mixed blocks” is an output. Each day should include three components. First, complete timed questions. Second, review misses using the taxonomy from earlier sections. Third, perform spaced recall of previous misses. This creates a closed loop. Questions reveal weaknesses. Review converts weaknesses into rules. Recall keeps rules available. Without all three, the plan becomes unstable. Use NBME timing only after the process has changed. If you take another NBME too soon, you may simply confirm the same plateau. Instead, use smaller validation tests during the two-week cycle. For example, after repairing renal physiology, do a timed set that includes renal but is not exclusively renal. If performance only improves when you know the topic is renal, transfer is incomplete. Step 1 does not announce the topic before each question. During the final days of the cycle, shift from learning mode to execution mode. Reduce passive content intake. Increase mixed timed blocks. Review your highest-yield rules. Practice pacing. Sleep consistently. Avoid resource changes unless a specific topic lacks any clear explanation in your current materials. Late resource switching can create anxiety and fragmentation. The checklist should be used at the end of each study day. If you cannot check an item, fix the process the next morning. Do not wait for the next NBME to reveal the same mistake. The most efficient students treat daily study as a feedback system. They do not merely accumulate hours. There is also a psychological benefit to a diagnostic plan. A stuck score can make students feel that nothing works. A pattern-based plan restores control because it defines the problem in solvable terms. Instead of saying, “I am bad at Step 1,” the student says, “I am repeatedly missing mechanism questions because I do not identify the pivot clue before reading answer choices.” That second sentence can be fixed. At the end of two weeks, compare performance with your starting diagnosis. Did the repeated errors decrease? Did timing improve? Did fragile corrects become more stable? Did mixed-block performance rise in the repaired domains? If yes, the plan is working. If not, return to the taxonomy. The failure may be deeper content, poor retrieval, or test anxiety that disrupts execution. Each requires a different response. Step 1 improvement is rarely a single dramatic breakthrough. It is usually the compound result of cleaner diagnosis, better retrieval, sharper reasoning, and more disciplined review. When those processes change, NBME performance has a stronger reason to move. Medically reviewed by: Jonathan Reyes, MD Use a diagnostic review system before adding another resource. Start with your last two self-assessments, classify every miss, and build the next week around the repeated failure patterns.Quick answer: Why is my Step 1 score not improving?
Start by Diagnosing the Plateau, Not Repeating the Same Plan
Separate Knowledge Gaps From Reasoning Errors
Miss Type
Typical Sign
Best Repair
One-Sentence Rule Format
Pure content gap
You did not recognize the disease, pathway, organism, or drug.
Rebuild the topic, then test it with active recall within 24 hours.
When I see [clue], think [diagnosis or mechanism] because [reason].
Mechanism translation gap
You knew the fact after reading the explanation but could not connect it during the question.
Write clue-to-mechanism links and drill similar questions.
[Clinical clue] points to [pathway defect], so the answer is [mechanism].
Distractor selection
You picked an answer that was true but not most supported.
Identify the decisive clue and the trap clue.
Do not choose [trap] unless [required discriminator] is present.
Stem-task error
You answered diagnosis when the question asked pathophysiology, adverse effect, or next mechanism.
Circle the final task mentally before reviewing answer choices.
The last sentence asks for [task], so eliminate answers in the wrong category.
Timing compression
Accuracy falls late in blocks or after long vignettes.
Use timed mixed blocks and a pacing checkpoint.
If time pressure rises, read the final sentence first and anchor the task.
Audit Your NBME Data Like a Clinician Reviews a Case
Trend the Score
Localize the Pattern
Name the Failure
Prescribe the Fix
Do not just review your NBME misses. Re-test the pattern that caused them.
Understanding a miss is not the same as repairing it.
Repair the Review Loop That Keeps Scores Stuck
The 5-Minute Miss Review
Use Active Recall and Spacing Instead of Passive Re-Exposure
Day
Primary Work
Recall Work
Plateau Target
Monday
Timed mixed block plus review
Create rules from misses
Identify current failure pattern
Tuesday
Targeted content repair
Retrieve Monday rules without notes
Close content gaps
Wednesday
Timed block focused on weak systems
Apply rules to related questions
Test transfer
Thursday
Mixed questions under pacing rules
Review older missed-question cards
Improve exam stamina
Friday
Reasoning audit of hardest misses
Rewrite vague rules
Reduce repeat mistakes
Weekend
Longer mixed set or self-assessment when appropriate
Consolidate top rules
Validate improvement
Rebuild Question Strategy for NBME-Style Reasoning
Task Anchor
Pivot Clue
Trap Check
Build a Two-Week Recovery Plan and Rapid-Review Checklist
Rapid-Review Checklist
References
Next Step
USMLE Step 1
Step 1 Score Not Improving? How to Diagnose Why Your NBME Scores Are Stuck
For NBME score plateaus and review
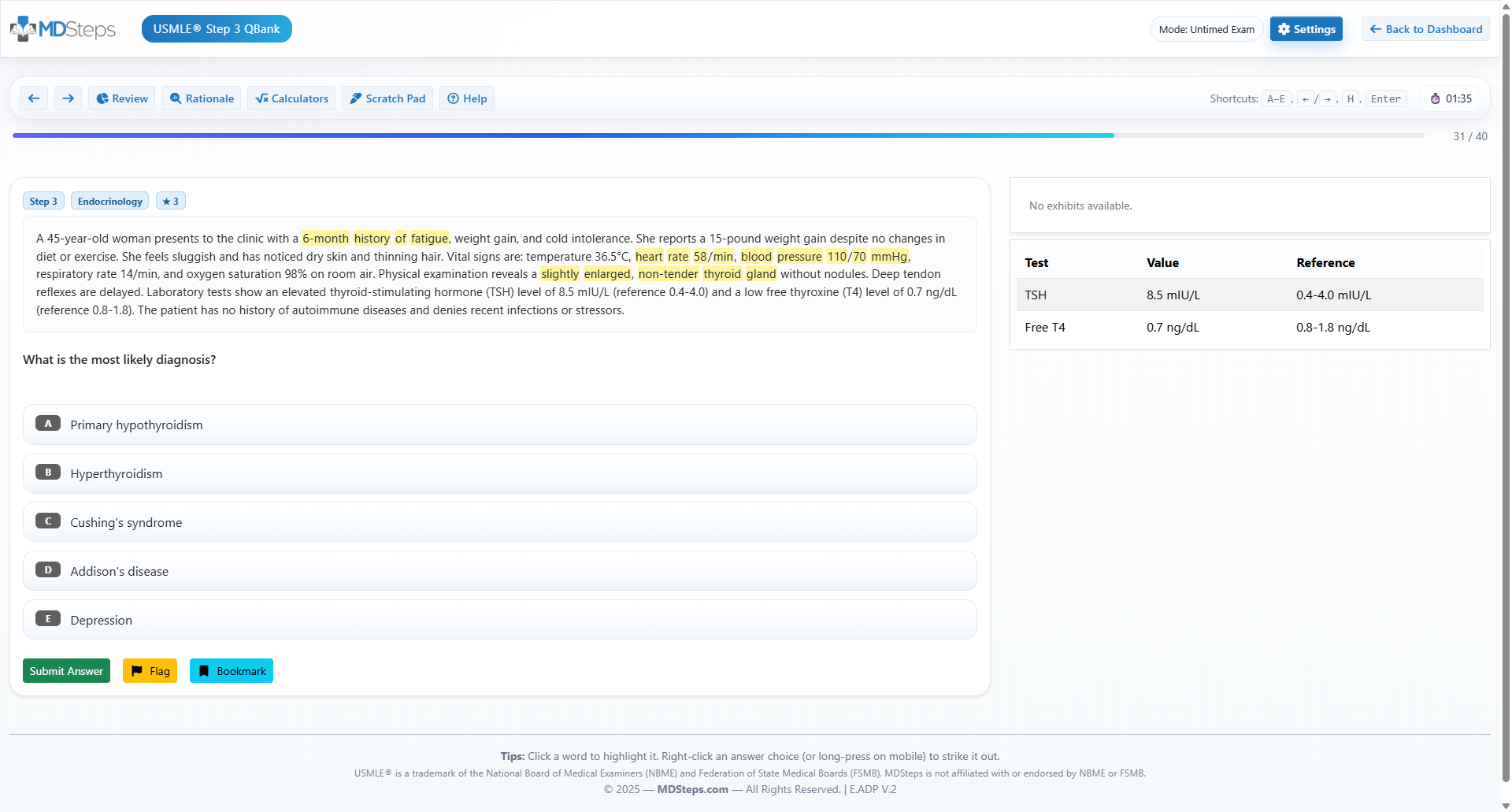
An NBME score report tells you what dropped. MDSteps helps show why it dropped.
Use MDSteps to sort NBME misses by weak system, reasoning trap, timing issue, distractor pattern, and readiness risk—then practice similar stems before your next assessment.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.
Practice-exam repair
Turn missed NBME concepts into targeted blocks instead of passive note review.
Pivot-clue review
Identify the clue that should have changed your answer before the choices pulled you away.
Readiness tracking
See which weak areas and miss patterns still need work before another assessment.
Step 1 Strategy
NBME Plateau Diagnosis
Core principle: A plateau is a data problem before it is a motivation problem. Your next study plan should be built from your missed-question pattern, not from a generic calendar.
Step 1
Step 2
Step 3
Step 4
NBME score stuck?
Practice-exam repair loop
NBME-style practiceMiss-pattern reviewTargeted weak-area blocks
Start with a free reasoning review. Full access includes NBME-style blocks, analytics, flashcards, Step 3 CCS, and study planning.
After NBME review
Still missing the same kinds of questions?
Read why that happens.
MDSteps workflow note: The analytics and exam readiness dashboard can help students identify whether misses are clustering by system, task, or repeated behavior. Use that information to build the two-week repair cycle rather than guessing where to spend time.