Mastering internal medicine on Step 2 CK demands more than memorizing guidelines—it’s about recognizing patient patterns and executing management decisions under time pressure. This guide distills the most high-yield internal medicine cases, combining diagnostic and management reasoning with Step 2 CK–specific logic. Roughly half of Step 2 CK questions stem from internal medicine. These cases integrate pathophysiology with applied reasoning—linking symptoms, labs, and imaging to first-line treatments. High-yield cases aren’t random: they represent common inpatient and outpatient patterns (acute coronary syndrome, DKA, pneumonia, AKI, sepsis). Understanding these archetypes is crucial because they appear as variable-length case stems that test clinical prioritization, not rote recall. Internal medicine’s breadth makes structured reasoning essential. For example, in chest pain, Step 2 CK expects you to differentiate pericarditis from myocardial ischemia using physical findings and ECG clues—and then select appropriate next steps (e.g., serial troponins, not emergent echo). Each correct answer relies on matching a real-world diagnostic flow to Step 2’s hierarchy of “most appropriate next step.” The MDSteps Adaptive QBank models these patterns using over 9000 case-based questions with dynamically evolving vignettes. Each miss creates flashcards and analytics that guide focused review, ensuring you don’t just memorize—but think like a resident on rounds. Chest pain is Step 2 CK’s classic multi-diagnosis case. The exam will test your ability to triage and interpret data quickly. A 58-year-old man with pressure-like pain radiating to the arm, diaphoresis, and risk factors—ACS. Sharp pleuritic pain worse with inspiration or lying flat, diffuse ST elevation—pericarditis. Sudden dyspnea, tachycardia, and pleuritic pain after surgery—pulmonary embolism. Management prioritizes stabilization first, diagnosis second. Step 2 CK rewards recognizing the most urgent rule-out (ACS, PE) before narrowing to less emergent etiologies. Practicing timed cases in MDSteps simulates this decision logic under the same 90-second-per-question pressure. Dyspnea questions blend physical findings, CXR interpretation, and oxygen strategy. An elderly smoker with wheezing and CO₂ retention points toward COPD exacerbation—management includes oxygen targeting 88–92% and nebulized bronchodilators. Orthopnea, rales, S3, and pulmonary congestion on CXR? Think acute decompensated heart failure—give IV diuretics and monitor urine output. Fever, productive cough, and focal crackles with consolidation—bacterial pneumonia, start empiric antibiotics after CXR confirmation. Step 2 CK often inserts subtle traps, such as offering a CT chest before basic stabilization or oxygen titration. The correct answer sequence follows: stabilize → confirm diagnosis → treat. MDSteps’ “vitals-first” reasoning mode trains you to identify these sequencing priorities automatically. Practice management decisions, CCS sequencing, live vitals, and weak-area review from one dashboard. Hospital-acquired infections are prime internal medicine Step 2 CK fodder. Key temporal clues: within 48 hours (likely non-infectious or catheter-related), after 72 hours (pneumonia, UTI, or line infection). The exam expects a diagnostic algorithm mindset: Understanding stewardship principles is key: Step 2 prioritizes evidence-based management and cost-effectiveness. Practicing these algorithms in MDSteps’ analytics dashboard reveals personal biases toward overtreatment or undertriage—both costly errors on exam day. Step 2 CK loves differential refinement: appendicitis vs diverticulitis vs cholecystitis. Distinguish by quadrant and systemic clues. For example, right lower quadrant pain after anorexia and mild leukocytosis—appendicitis. Left lower quadrant with fever in an older adult—diverticulitis. Right upper quadrant, postprandial pain, positive Murphy’s sign—cholecystitis. Step 2 may present atypical cases (e.g., elderly diabetic with minimal tenderness), testing recognition of subtle cues rather than textbook presentations. Management hierarchy: assess stability → rule out perforation → imaging (CT or US) → antibiotics or surgery. Every Step 2 internal medicine case rewards prioritizing life-threatening conditions first and definitive imaging later. MDSteps’ integrated flashcards highlight “next best test” logic across hundreds of similar stems, reinforcing adaptive reasoning rather than rote recall. Syncope and shock questions assess triage skills. Vasovagal (preceded by nausea, benign). Orthostatic (volume loss). Cardiogenic (history of MI, S3). Arrhythmic (sudden, no prodrome). Step 2 CK’s correct answer often depends on initial management—not final diagnosis. Always start with ABCs, EKG, and vitals before advanced imaging. In shock questions, memorize these vital sign patterns: Recognizing the physiologic pattern saves time—critical when 10% of Step 2 CK cases hinge on shock management. MDSteps analytics track your average time-to-correct for these cases, highlighting cognitive choke points before test day. Students often separate “diagnosis” and “treatment” in their study routines, but Step 2 CK merges them. You’ll need to reason forward (what’s next) and backward (what did I miss). The best approach: deliberate practice. Use MDSteps’ Study Plan Generator to schedule system-based case blocks (e.g., cardio, pulm, renal) while alternating diagnostic (pattern recognition) and management (algorithmic response) sessions. For reinforcement, review errors by creating an adaptive flashcard deck of missed management questions. Spaced repetition ensures recall under fatigue. Combine this with simulated NBME pacing (40-question blocks, 1 hour) to build endurance and decision stability. Internal medicine success depends less on memorized minutiae and more on consistency across evolving presentations. Internal medicine’s complexity is an opportunity: every case reinforces a repeatable diagnostic pattern and evidence-based management chain. Build these habits daily with MDSteps’ adaptive analytics and personalized study plans—because Step 2 CK doesn’t just assess what you know, but how you think under pressure. References:Why Internal Medicine Dominates Step 2 CK
Case 1: Chest Pain – ACS, Pericarditis, or PE?
Feature ACS Pericarditis PE Pain character Pressure Pleuritic Pleuritic ST changes Localized elevation/depression Diffuse elevation + PR depression Sinus tachy, S1Q3T3 (rare) Next step ECG + troponins NSAIDs, echo if tamponade CT pulmonary angiogram Case 2: Dyspnea – CHF, COPD Exacerbation, or Pneumonia?
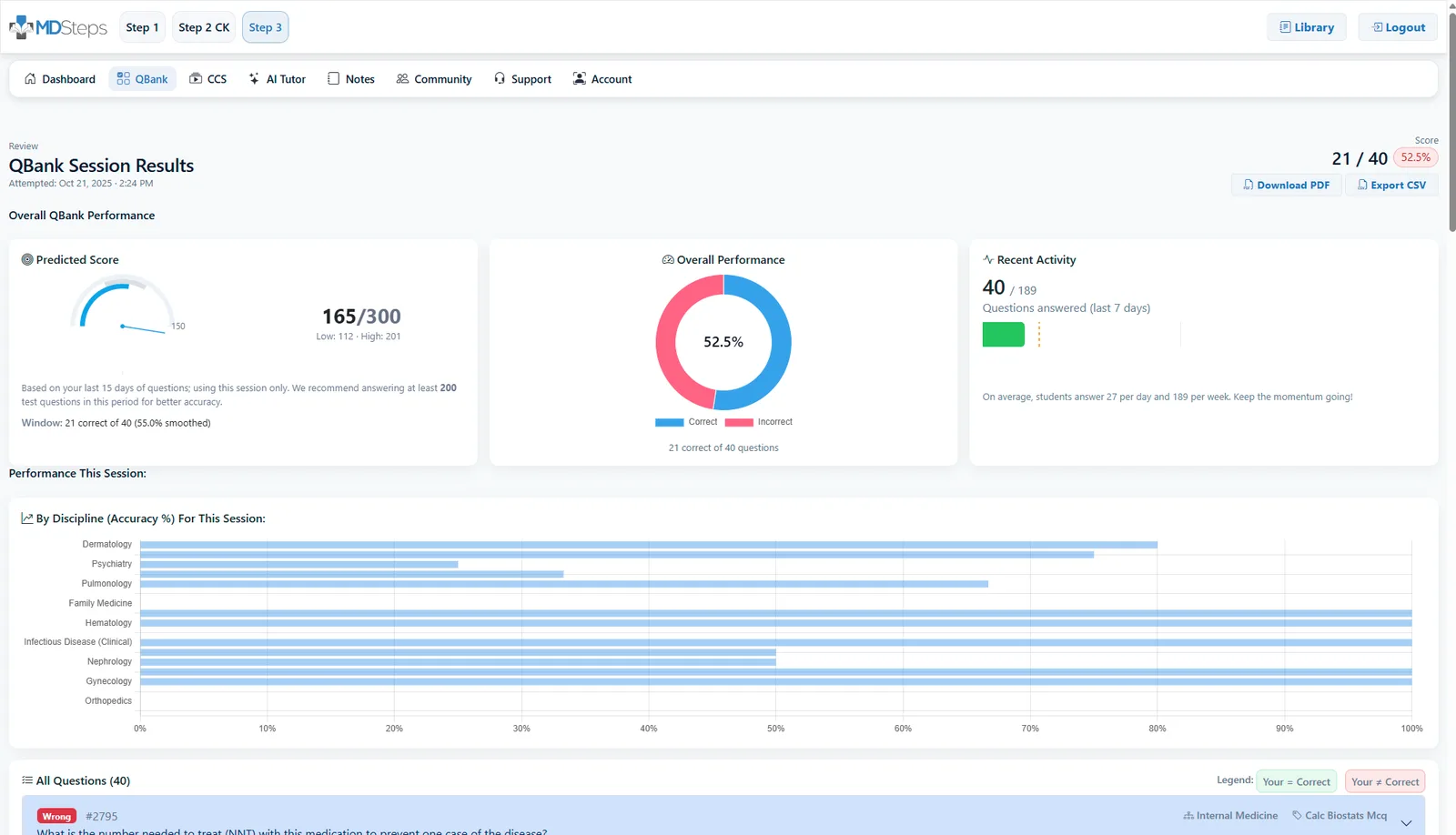
Turn this into Step 3 + CCS practice
Practice the sequence, not just the diagnosis.
See how it works
Case 3: Fever in a Hospitalized Patient
Case 4: Abdominal Pain – Acute Abdomen Logic
Case 5: Syncope and Shock – Rapid Pattern Recognition
Type BP HR Skin Key clue Hypovolemic ↓ ↑ Cool Trauma, GI bleed Cardiogenic ↓ ↑ Cool MI, JVD, crackles Distributive ↓ ↑ Warm Sepsis, anaphylaxis Integrating Diagnostics and Management in Study Practice
Rapid-Review Checklist: Internal Medicine Case Mastery
1. NBME Step 2 CK Content Outline (USMLE, 2024).
2. Harrison’s Principles of Internal Medicine, 21st Edition.
3. American College of Physicians Clinical Guidelines (ACP, 2024).
4. MDSteps Internal Medicine QBank & Analytics Dashboard.
USMLE Step 2 CK
Internal Medicine High-Yield Cases for Step 2 CK

Full access: $27/mo
Lifetime: $299
135 CCS casesStep 3 QBankManagement reasoning
Monthly access. Cancel anytime. No free trial required.
CCS workflow