Understanding Step 3 Demands as an IMG on Rotations
As an international medical graduate, you have a unique challenge: you must build a serious Step 3 study schedule for IMGs while navigating clinical rotations, new systems, and often a new country. Step 3 is a two-day exam focused on independent practice, clinical decision-making, and patient safety. It combines high-volume multiple-choice questions with computer-based case simulations (CCS), and many questions assume you are already managing a busy inpatient list or clinic panel. That means your prep must mirror that reality: decisions under time pressure, tracking data across several notes, and prioritizing among competing tasks.
IMGs frequently report three major constraints: unpredictable rotation hours, cognitive fatigue from working in a second language or system, and the pressure to prove themselves on the wards. Your study plan has to respect all three. Instead of imagining a perfect, uninterrupted 8-week “dedicated” period, it is far more realistic (and protective of your mental health) to build a rotation-compatible plan: one that assumes nights, long calls, and sudden schedule changes, and still moves you forward.
Think of Step 3 prep as an additional longitudinal “clinic” you are managing. Your “patients” are domains: internal medicine, pediatrics, OB/GYN, psychiatry, surgery, preventive medicine, ethics, and biostatistics/epi. Each domain needs repeated follow-up: initial assessment (baseline performance), active treatment (questions, CCS, and review), and maintenance (spaced repetition and mixed blocks). If any domain is “lost to follow up,” it will show on your score report.
Before you even open a question bank, define the non-negotiables in your life:
- Rotation commitments: start/end times, call days, post-call days, clinic vs ward intensity.
- Commute time and sleep requirements (aim for a minimum of 6–7 hours on most nights).
- Visa or licensing deadlines that dictate the latest date you can safely take Step 3.
- Personal obligations (family, childcare, religious observances) that are not optional.
Only after mapping those constraints should you build your Step 3 calendar. Many IMGs make the mistake of starting with a generic “do 40 questions daily” goal and then trying to squeeze it into a 14-hour day on the wards. That approach predictably fails, leading to guilt and burnout. Instead, we will construct a plan that starts from your real schedule, allocates a modest but consistent daily study dose, and then layers in higher-yield “pushes” during lighter weeks.
Finally, remember that Step 3 is not just about raw medical knowledge. It rewards:
- Prioritization and triage: which task is most urgent for patient safety.
- Next best step logic: ordering tests and treatments in rational sequence.
- Ambulatory and public health thinking: screening, counseling, and follow-up.
- Data interpretation: guidelines, risk calculators, and evidence summaries.
Your study schedule should therefore allocate time not only for questions, but also for reflecting on why each option is right or wrong, and how you would manage a similar patient during your actual rotation. When your study time is limited, depth of processing matters more than sheer volume; a well-analyzed 20-question block can be more valuable than 60 rushed questions done half-asleep after call.
Clarifying Your Timeline, Baseline, and Score Goal
The next step in building a realistic Step 3 study schedule for IMGs is to define three things: timeline, baseline, and target.
The next step in building a realistic Step 3 study schedule for IMGs is to define three things: timeline, baseline, and target. Without these anchors, it is impossible to know whether your plan is feasible.
1. Timeline: when should you take Step 3?
Start by mapping out the next 6–9 months. Mark rotation blocks, vacations, visa or licensing deadlines, and residency application milestones. Identify:
- Heavy rotations: ICU, night float, ED, or busy inpatient blocks.
- Lighter blocks: electives, clinic-heavy rotations, research time.
- Protected windows: any 3–7 day stretches where you can be off or have minimal duties.
Most IMGs can reach a solid Step 3 performance with about 8–12 weeks of consistent, rotation-compatible study (not “dedicated” monastic study), plus a short ramp-up in the final 2–3 weeks. If your schedule is extremely demanding, plan on the longer side and lean more heavily on daily micro-sessions and spaced repetition.
2. Baseline: where are you starting?
If you have not touched Step 2-level material in over a year, your first move should be a diagnostic assessment. This can be:
- An NBME or other reputable self-assessment approximating Step 3 difficulty.
- A mixed set of 80–120 timed questions from a high-quality Step 3 question bank.
Take this baseline under exam-like conditions: timed, minimal interruptions, and no consulting notes mid-block. Do not obsess about the score; you are mainly looking for pattern recognition:
- Are you missing questions due to knowledge gaps or test-taking errors?
- Do you struggle more with ambulatory, OB/GYN, or peds content?
- Are you often running out of time on blocks?
Record your baseline in a simple tracking sheet: date, resource, % correct or scaled score, and 3–5 key themes from your error review. This will be your “before” picture.
3. Target: what is a realistic goal?
Step 3 is a pass/fail gate for licensure, but many programs (and visas, fellowships, or competitive hospitals) still informally care about performance. Define:
- A minimum acceptable target (clear pass, no anxiety about repeating).
- An ideal aspirational range that represents your best realistic performance.
Avoid magical thinking. If you are currently at a low baseline and working 70–80 hours per week, aiming for a massive score jump in six weeks will only create pressure and disappointment. Instead, align your target with your available time and mental bandwidth. You can always improve over time with additional practice exams or focused revisits to weak areas.
Once timeline, baseline, and target are clear, you can make evidence-based tradeoffs: how many question blocks per week, how often to do CCS practice, and how much time to allocate to review versus new material. In the next sections, we translate those tradeoffs into a weekly template that respects your rotation schedule.
Designing a Rotation-Friendly Weekly Template
Now it is time to convert your abstract Step 3 study schedule for IMGs into something concrete: a weekly template that you can reuse and slightly modify for each rotation.
Now it is time to convert your abstract Step 3 study schedule for IMGs into something concrete: a weekly template that you can reuse and slightly modify for each rotation. The goal is not perfection; it is consistency. A stable minimum dose of high-quality questions and targeted review beats sporadic “marathon” days followed by long gaps.
Start by categorizing your weeks into three intensity levels:
- Green weeks: lighter rotations, no call or infrequent call, early finishes.
- Yellow weeks: moderate workload, some call, occasional late nights.
- Red weeks: ICU, nights, ED, or heavy inpatient with frequent call.
Each category will have a different “dose” of Step 3 work. For example, during green weeks you might target 200–240 questions plus CCS practice; during red weeks, your minimum effective dose might be 80–100 targeted questions plus quick flashcard review.
| Day | Before Work | After Work | Total Questions | CCS / Review Focus |
|---|---|---|---|---|
| Mon (post-call) | Sleep / Recovery | Light review of 10–15 marked questions | 10–15 | Skim explanations, no new CCS |
| Tue | 10 timed questions (30–40 min) | 20 questions + review (60–75 min) | 30 | 1 short CCS case, focus on orders |
| Wed | Spaced flashcards (15–20 min) | 30 mixed questions, full review | 30 | Ambulatory & prevention topics |
| Thu | 10–15 questions (timed) | CCS practice + review of key management steps | 10–15 | 2 CCS cases (inpatient + outpatient) |
| Fri | Rest or short flashcard session | 20–25 questions, prioritize weak areas | 20–25 | Review missed questions from week |
| Sat | 40–50 question block + deep-dive review (2.5–3 hours) | 40–50 | Mix of specialties, 1 CCS case | |
| Sun | Light review, flashcards, planning next week (60–90 min) | 0–10 | Schedule, meta-review, rest | |
Use this matrix as a starting point. Slot your real shift times into the “Before Work” and “After Work” columns. Be honest: if you rarely function before 6 a.m., do not build a schedule that depends on pre-rounds study. Similarly, if you know that after a 14-hour shift you are cognitively done, keep post-shift tasks short and low-friction (flashcards, revisiting missed questions, or a single short CCS case at most).
For each week, define:
- Question target: total number of questions and average per day.
- CCS target: number of full cases or “mini-cases” to run.
- Review blocks: specific windows for deeper explanation reading and note-making.
At the end of every Sunday, quickly audit the week: Did you hit 70–80% of your goals? If yes, you are on track. If not, adjust the coming week’s goals downward slightly; a plan you actually follow is more powerful than an ideal plan that exists only on paper.
Daily Micro-Schedules: Time Blocking and Cognitive Load
Weekly matrices are helpful, but success on Step 3 while on rotations is determined by your daily micro-schedule.
Weekly matrices are helpful, but success on Step 3 while on rotations is determined by your daily micro-schedule. As an IMG, your cognitive load is already high: you are often thinking in multiple languages, adapting to new electronic health records, and decoding the unspoken culture of your team. Your Step 3 plan must avoid overloading you further.
A simple daily structure you can reuse:
- Micro-block 1 (pre-work or commute, 20–30 min): flashcards or 5–10 questions.
- Micro-block 2 (midday, 10–15 min): one or two explanations from the morning, or a quick CCS review.
- Core block (after work, 45–90 min): a 10–20 question timed set plus deliberate review.
Notice that only one block is really “heavy.” The others are maintenance and consolidation. This spacing helps your brain re-encounter concepts across the day, strengthening memory without requiring huge time chunks.
To keep cognitive load manageable:
- Limit decision fatigue. Decide once, in advance, what each day’s blocks will cover (e.g., “Tuesdays = ambulatory + OB/GYN”). Avoid nightly re-planning.
- Batch similar tasks. Do questions in one window, explanation reading in another, and flashcards in a third. Multitasking across modes increases effort without improving learning.
- Use focused, timed sprints. For example, 25 minutes of pure questions followed by 5 minutes of stretching and hydration, then 25 minutes of review.
- Protect sleep. Chronic sleep debt blunts your ability to form long-term memories and process complex vignettes. If you are consistently sleeping <6 hours, reduce question load temporarily and prioritize rest.
You can implement this daily micro-schedule with something as simple as calendar events on your phone. Color-code your Step 3 blocks differently from clinical duties so you can see, at a glance, where your exam prep fits. For IMGs who feel overwhelmed by the U.S. system’s pace, this visual reminder can be reassuring: you are not just “hoping” to study; you have a realistic, pre-committed plan.
Example “Yellow Day” Micro-Schedule (Ward Month)
- 06:30–06:50: Coffee + 6–8 flashcards and 3–5 quick questions.
- 07:00–17:30: Rotations (quickly jot down any puzzling cases to look up later).
- 18:30–19:15: 10–12 mixed questions, fully timed.
- 19:15–19:45: Review explanations for all questions, mark key pearls.
- Before bed (5–10 min): Scan your notes, select 2–3 “must remember” points.
This kind of daily plan is what allows you to accumulate hundreds of high-quality questions and dozens of CCS cases over weeks, even when no single day feels particularly heroic.
Integrating Question Banks, CCS Cases, and Spaced Repetition
Once your weekly and daily templates are set, the question becomes what to put into those blocks.
Once your weekly and daily templates are set, the question becomes what to put into those blocks. For Step 3, your core tools are: high-quality question banks, CCS case practice, and some form of spaced repetition for facts and algorithms.
1. Question banks: how many and how to use them
For most IMGs, it is safest to commit deeply to one primary Step 3 question bank and, if time permits, selectively draw on a second resource for extra exposure. Doing multiple Qbanks superficially is less useful than mastering one with deliberate review. Aim to:
- Do most blocks in timed, random mode to simulate exam conditions.
- Reserve a small fraction (10–20%) for tutor mode on particularly weak topics.
- Spend at least as much time reviewing explanations as you do answering questions.
When you review, focus on extracting transferable patterns: “In an otherwise healthy young woman with chest pain and normal ECG, what features push me toward anxiety vs PE vs costochondritis?” Capture these in brief notes or flashcards, not long paragraphs.
High-yield QBank habits
- Always answer under timed conditions.
- Tag questions by mistake type (knowledge vs process).
- Re-do difficult blocks after 2–4 weeks.
- Track running % correct by system and task.
Common QBank pitfalls
- Reading explanations passively without summarizing.
- Ignoring ambulatory and preventive care questions.
- Rushing blocks after exhausting shifts.
- Never revisiting missed questions.
A platform like MDSteps can streamline this by using an adaptive Step 3-style QBank that focuses on your weak areas, automatically generating flashcard-ready “missed question” decks and tagging content by system and task. That kind of automation is particularly helpful for IMGs who do not have time to manually categorize every error while juggling rotations.
2. CCS cases: weaving simulations into a busy week
Many IMGs postpone CCS practice until the very end, then panic when they realize the interface and pacing feel unfamiliar. Instead, schedule CCS from the beginning:
- Start with 1–2 cases per week, focusing on basic order sets and timing.
- Gradually increase to 3–5 cases per week in the final month.
- Alternate inpatient and outpatient scenarios to cover both Day 2 styles.
Treat each CCS case as a story: chief complaint, immediate stabilization, diagnostic workup, treatment, counseling, and disposition. After each case, ask: “What did I do too late? What did I forget? Did I over-order or under-treat?” This reflection is where learning happens.
If you have access to MDSteps’ live vitals CCS cases with realistic physiology and timed orders, you can mirror exam dynamics more closely: watching vitals change as you intervene reinforces correct management sequences and helps you feel less anxious when you encounter similar dynamics on test day.
3. Spaced repetition for consolidation
Finally, reserve a small daily slot for spaced repetition. This does not need to be complicated: 10–20 minutes of flashcards built from your missed questions and key algorithms is enough. Focus on:
- Management algorithms (e.g., chest pain, DKA, hypertensive emergency).
- Screening ages and intervals (breast, colon, cervical cancer, etc.).
- Drug monitoring, contraindications, and major side effects.
- Classic “can’t miss” red-flag presentations.
Many IMGs find it time-saving to let software generate cards from explanations. MDSteps, for example, can automatically create decks from your incorrect questions and export them to Anki, preserving a spaced-repetition rhythm even when your rotation schedule is chaotic.
Adapting Your Plan for Heavy Rotations, Call, and Burnout Risk
Even the best Step 3 study schedule for IMGs will collapse if it does not anticipate bad weeks.
Even the best Step 3 study schedule for IMGs will collapse if it does not anticipate bad weeks. Heavy rotations, night float, and acute life events are not “if,” they are “when.” Your plan must include explicit rules for these situations.
1. Red-rotation rules: minimum effective dose
During ICU, night float, or ED months, define a minimum effective dose of Step 3 work:
- On work days: 5–10 questions or 10–15 minutes of flashcards, maximum.
- On post-call days: no new content; at most, skim a few previously missed questions.
- On days off: one slightly larger block (20–30 questions plus brief review).
This keeps the material “warm” without exhausting you. Importantly, write this policy down before the rotation starts, so you do not criticize yourself for not doing 40 questions after a 28-hour call.
2. Protecting mental health and energy
Burnout is a significant risk during this phase. Warning signs include emotional detachment from patients, cynicism, difficulty concentrating on questions you would normally get right, and feeling hopeless about your score. If you notice these, step back:
- Reduce study volume for 1–2 weeks and prioritize sleep, nutrition, and brief exercise.
- Talk to a trusted colleague, mentor, or counselor about workload and coping strategies.
- Consider pushing the exam date if your functioning is consistently impaired.
Remember: a two- or three-week delay to preserve mental health is almost always better than taking Step 3 under severe burnout and risking a fail that follows you for years.
3. Handling schedule shocks
Schedule shocks—unexpected extra calls, sick coverage, or family emergencies—are inevitable. When they happen, apply a simple triage algorithm:
- Stop and acknowledge the change rather than clinging to the old plan.
- Re-classify the week as red or yellow based on new workload.
- Reset goals (for example, cutting question volume by 30–50%).
- Salvage small wins (flashcards on commute, 5–10 questions on lighter days).
The key mindset: your plan is a living document, not a contract. Flexible, iterative adaptation is a sign of professionalism, not failure.
Final Month Plan: Practice Exams, CCS Focus, and Analytics
In the last 4 weeks before Step 3, your schedule should shift from broad content acquisition to simulation and refinement.
In the last 4 weeks before Step 3, your schedule should shift from broad content acquisition to simulation and refinement. The questions you choose, the CCS cases you run, and how you use analytics all become more targeted.
1. Full-length simulations
Aim for at least 1–2 near-full-length practice days in the final month—ideally on off days or lighter weekends. Structure them to mimic the real exam:
- 6–7 timed blocks of mixed questions with realistic break distribution.
- A CCS “mini-session” after several blocks, to train cognitive switching.
- Strict phone and notification control.
After each simulation, do not immediately jump back into more questions. Instead, spend the next day (or two shorter sessions) doing focused review: identify which blocks or topics dragged your score down, which question stems you misread, and where fatigue showed up.
2. CCS-heavy weeks
In the last month, increase CCS exposure:
- Week –4 to –3: 3 cases per week.
- Week –3 to –2: 4–5 cases per week.
- Week –2 to –1: 5–7 cases per week (mixing new and repeated scenarios).
Focus on high-yield scenarios: chest pain, shortness of breath, altered mental status, OB triage, pediatric fever, and common outpatient follow-ups. Practice ordering vitals, monitoring parameters, consults, and patient counseling efficiently. Notice how often the best move is observation with close follow-up rather than aggressive intervention.
3. Using analytics to close gaps
At this stage, you should rely heavily on performance data rather than intuition. Track, by system and task:
- Which organ systems are below your target % correct.
- Which task types (diagnosis, next best step, ethics, preventive care) you miss most.
- Time per question and frequency of rushed last-minute guesses.
A platform with an exam readiness dashboard, like MDSteps, can be especially helpful: it can surface patterns you might not notice (for example, a consistent weakness in risk stratification questions or in pediatrics ambulatory care) and suggest specific blocks to shore up those gaps in your final weeks.
In the last 5–7 days, taper volume slightly. Maintain 20–40 questions per day with focused review, but reduce new topics. Prioritize:
- Previously weak systems that are now close to target.
- High-yield ethics, communication, and patient safety scenarios.
- Refreshing CCS interface familiarity and order sets.
Your goal is to enter exam week feeling practiced but not depleted.
Rapid-Review Checklist and Exam-Day Essentials for IMGs
Before you lock in your Step 3 study schedule around clinical rotations and boards, run through this rapid-review checklist.
Before you lock in your Step 3 study schedule around clinical rotations and boards, run through this rapid-review checklist. It will help ensure that your plan is realistic, comprehensive, and aligned with how Step 3 actually tests you.
A. Rapid-Review Planning Checklist
- Have you mapped your next 8–12 weeks with green, yellow, and red rotation weeks?
- Did you take a baseline self-assessment or large question block under timed conditions?
- Do you have a weekly question and CCS target tailored to each rotation type?
- Is your daily micro-schedule built around 2–3 predictable blocks (before work, midday, evening)?
- Are you protecting at least 1 day per week for deeper review and planning?
- Do you have a simple system for spaced repetition (flashcards or auto-generated decks)?
- Have you defined minimum effective dose rules for ICU, nights, and call-heavy months?
- Are full-length simulations and CCS-heavy weeks penciled into your final month?
- Do you have a way to track analytics by system, task type, and timing?
- Have you built recovery and mental health protection into your plan, not as an afterthought?
B. Exam-Day Essentials for IMGs
- Confirm your route, parking, and ID requirements several days in advance.
- Plan simple, familiar foods and hydration that will not upset your stomach.
- Practice your break strategy during simulations (when to snack, when to stretch).
- Bring layers—testing centers can be unpredictably cold or warm.
- Have a pre-exam wind-down routine: no last-minute cramming into the night.
- Use a brief breathing or grounding exercise just before each block.
- During CCS, prioritize stabilization, key diagnostics, and clear follow-up; do not chase every possible test.
- Remind yourself that imperfect performance on one block or case does not define your whole exam.
If you prefer structured support, you can mirror this entire framework inside a digital platform. MDSteps includes an automatic study plan generator keyed to your exam date and rotation intensity, an adaptive QBank with over 9,000 questions, live vitals CCS cases for Step 3, and an analytics dashboard that tracks your readiness by system and task. Combined with automatic flashcard decks built from your misses (exportable to Anki), this allows you to focus on thinking like an independent physician while the logistics of scheduling, tracking, and prioritizing are handled for you.
- USMLE. Step 3 Exam Content.
- USMLE. Step 3 Content Outline and Specifications.
- Federation of State Medical Boards (FSMB). USMLE Step 3 Overview.
- Young JQ, et al. Cognitive Load Theory: Implications for Medical Education. Med Educ.
- Yuan X, et al. Evidence of the Spacing Effect and Influences on Perceptions of Learning. Cell Rep.
- Summary of Spaced Repetition Principles (overview article).
- Si J, et al. Using Cognitive Load Theory to Tailor Clinical Reasoning Training. BMC Med Educ.
- Voice A. Spaced Repetition: Towards More Effective Learning in STEM. Phys Educ.
Alexandra Ortiz, MD, Board-Certified Internal Medicine.
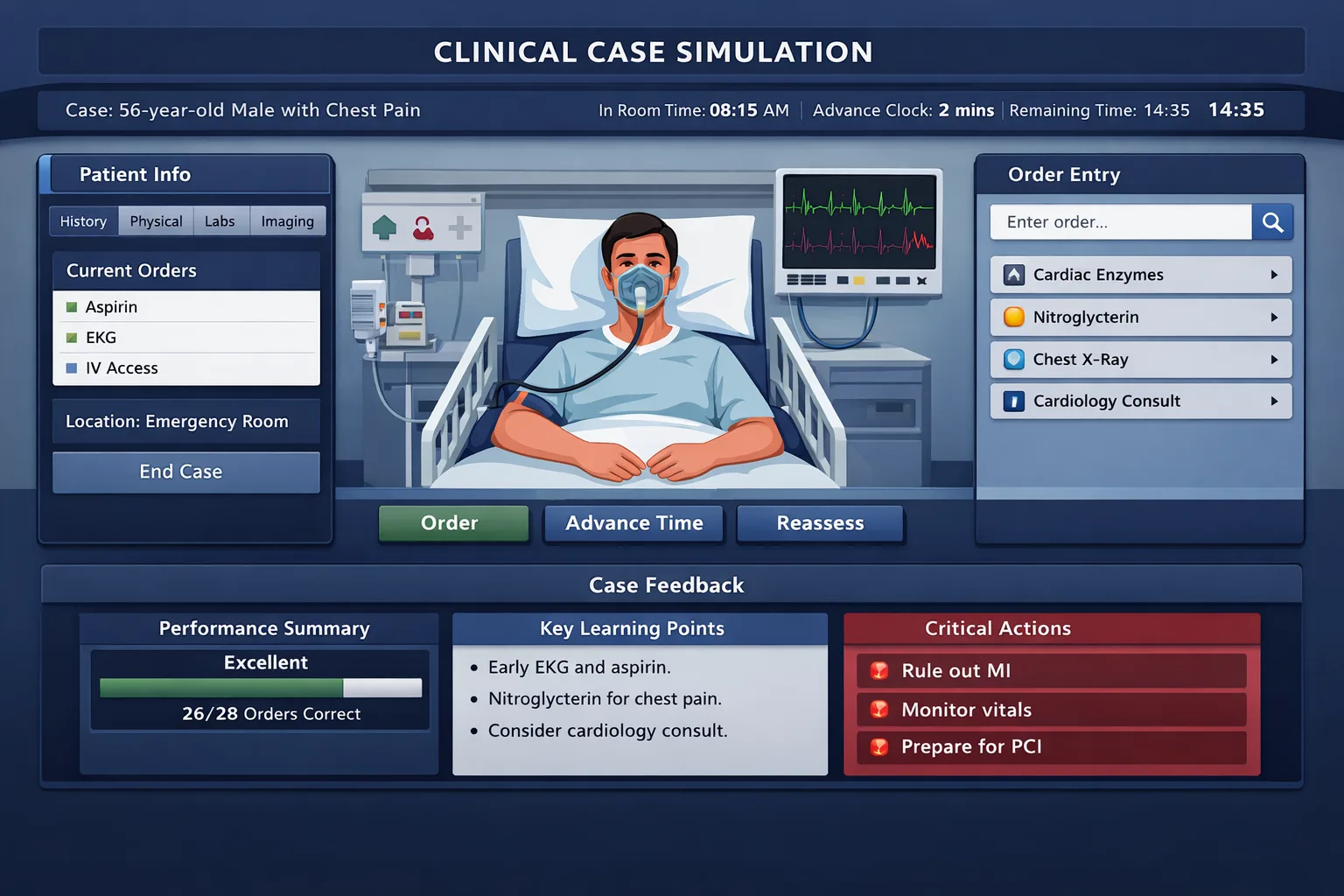
CCS is not just what you order. It is when you order, reassess, and close the case.
MDSteps helps you practice live CCS cases with vitals, orders, labs, time advancement, reassessment, closure, and after-action feedback.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.