Use timed orders, evolving vitals/labs, scorecards, and reasoning-focused review to train the exact CCS workflow: stabilize, order, reassess, advance time, and close safely. Cancel anytime. First month protected by our 7-day good-faith refund guarantee after 100 questions or 5 CCS cases.
If you’re searching for the best Step 3 CCS cases platform, you’re already asking the right question—but the
“best” option is rarely the one with the most cases. On Step 3, Computer-based Case Simulations (CCS)
reward sequencing, timing, and setting (clinic vs ED vs inpatient) as much as diagnosis.
A platform that forces you to practice those mechanics—free-text order entry, deliberate clock management,
and physiologic consequences—usually transfers better to test day than passive reading or static checklists.
The USMLE describes CCS as a dynamic simulation where patient status changes with simulated time and with
your management choices. You’re scored on indicated actions, their timing and sequence, and you lose points
for unnecessary or harmful actions. In other words: the “right” order late can be worth little, and the
“reasonable” order placed in the wrong setting can silently drag you down.
CCS platforms differ most in how they teach you to think under the clock. To compare them fairly,
this article uses a rubric built around the components the USMLE emphasizes: appropriate actions, correct
setting, and correct timing/sequence. We also weigh usability and feedback quality because they determine
whether you can iterate quickly across many cases.
Get full MDSteps access with NBME-style questions, reasoning-first explanations, analytics, flashcards, and CCS cases for one simple monthly price.
Below is a high-yield comparison of widely used CCS practice options. “Rank” reflects the rubric above and
prioritizes test-day transfer, not marketing claims. Costs and case counts can change, so treat those as
directional and verify on the vendor site.
*Ranking reflects exam-transfer features (timing/sequence, setting, physiologic consequences, feedback quality).
Different budgets and timelines may shift what’s “best” for you.
A CCS simulator is only as useful as the habits it builds. This section translates platform features into
Step 3 scoring behaviors: what you’ll do faster, what you’ll stop over-ordering, and what you’ll learn to
recognize early. Use it to pick the tool that fixes your weak links.
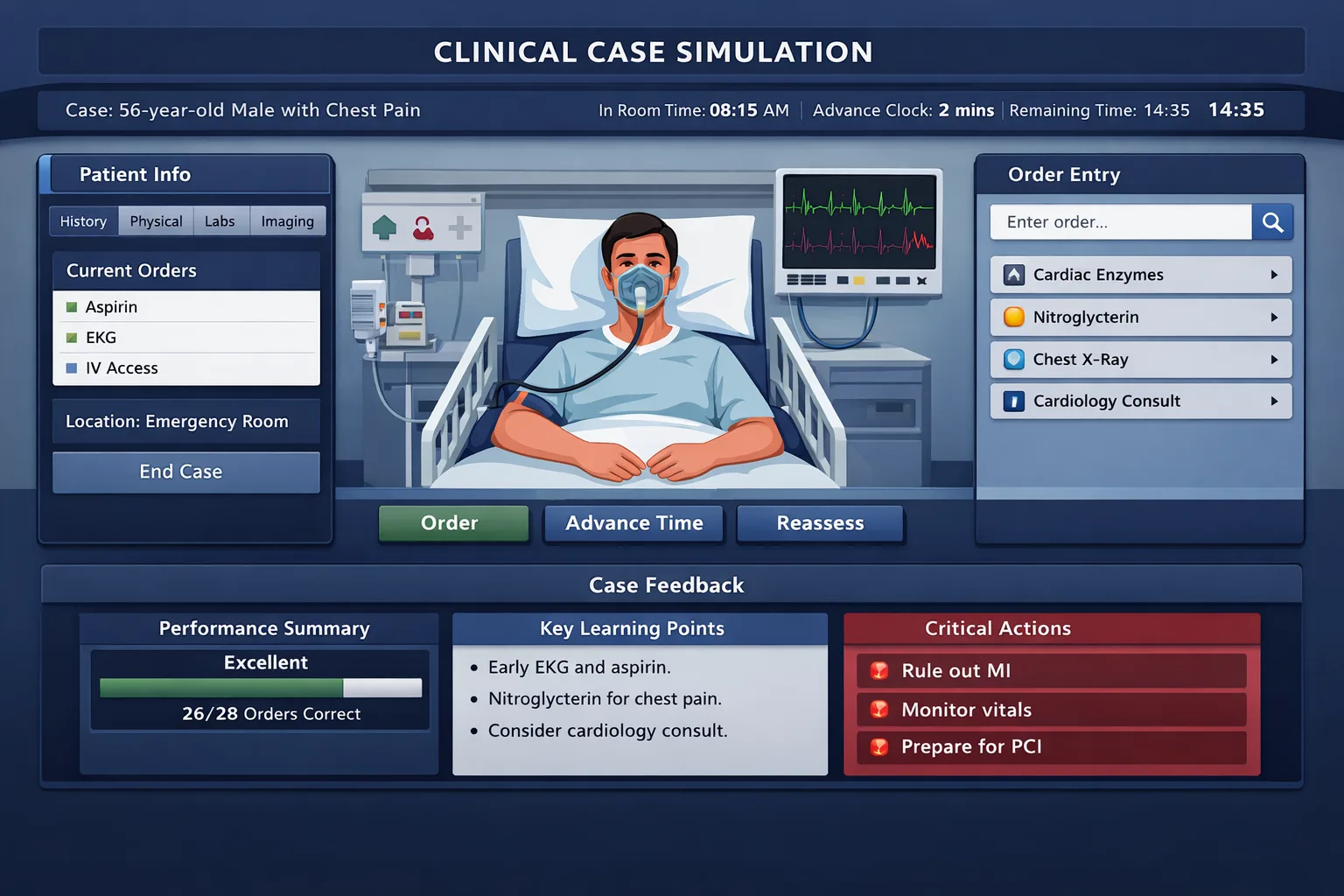
MDSteps’ differentiator is that cases behave like a living patient: vitals, labs, and trajectories
evolve as you intervene, and the platform emphasizes timed orders—a subtle but crucial
behavior on the real exam. That matters because CCS scoring is heavily influenced by whether your
management was not only correct, but correct in sequence. Practicing in a system that forces
you to “treat → reassess → advance time” makes timing feel natural instead of forced.
The other high-yield difference is feedback granularity. A robust scorecard should tell
you: what you did right, what you missed, what was unnecessary, and what to change next time. In CCS,
the fastest way to improve isn’t doing 100 random cases—it’s identifying your recurring misses
(forgetting DVT prophylaxis on inpatients, delaying antibiotics in sepsis, failing to pick the correct
setting, forgetting repeat vitals/monitoring) and drilling them until they disappear.
If you’re already strong on diagnosis but bleed points on timing, monitoring, or disposition,
this style of physiologic practice tends to give the best return per case. (MDSteps also pairs well
with a question bank—CCS success is workflow + knowledge, not one or the other.)
CCSCases.com is popular because it offers a large bank (170+ publicly advertised) and a simulator that
aims to feel close to the real interface, with a large order list (20,000+ orders advertised). That
combination is ideal for one thing: repetition. Repetition builds speed, and speed is the
currency of CCS because you need time to treat, reassess, and safely close out the case.
Where high-volume tools sometimes underdeliver is in coaching you on why you lost points.
Many learners can identify “missed orders” but still fail on the exam because their order sequence and
timing are off. If you use CCSCases.com, your goal should be to treat it like a driving simulator:
build interface instincts and a standard workflow, then deliberately audit timing and disposition.
Best use: early to mid prep, when you need repetition to make the software feel automatic and expand
your “order vocabulary” so you’re not hunting for common items.
UWorld’s advantage is integration: many learners already use it for Step 3 MCQs, so the CCS component
fits naturally into the same daily routine. UWorld also emphasizes free-text order entry, which is
important because the real CCS clerk recognizes orders in multiple typed forms and prompts you based on
the first characters entered.
UWorld’s explanations can be excellent for connecting a presentation to a management plan. Where some
learners struggle is translating that knowledge into a tight CCS tempo: early stabilization, minimal
diagnostic steps that change management, and clock advancement with a defined purpose. If you choose
UWorld CCS as your main simulator, be explicit about building a case script so you don’t
spend your real time reading instead of managing.
Best use: as a convenient primary tool for learners who thrive on explanation-rich review and want one
platform for MCQ + CCS, supplemented by official sample cases for calibration.
MasterCCS markets real-time scoring and detailed feedback during and after cases. For some learners,
real-time cues accelerate habit change—especially for timing/sequence. Because “newer” platforms can
vary in maturity, treat them as promising add-ons and verify that case breadth and interface behavior
match what you need.
Regardless of what you buy, the official USMLE/Primum practice materials remain non-negotiable: they
calibrate your expectations for how the real clock behaves, how the clerk recognizes orders, and how
cases end. The official cases are not enough for mastery, but they are the closest thing to a “true
interface check” you’ll get before test day.
Finally, resources like AMBOSS are valuable for Step 3 MCQs, but they are not CCS simulators. Treat them
as knowledge multipliers, not substitutes for interactive case reps.
The “right” simulator depends on how much time you have and what type of errors you make. Use the scenarios
below to pick a setup that fits your constraints without overbuying. The goal is a tight feedback loop:
do a case → identify a recurring error → drill that error on the next case.
MDSteps note (one-time): if you want a simulator that actively trains timing/sequence with evolving vitals and then
shows you a robust scorecard of recurring misses, MDSteps’ CCS runner is built for that feedback loop.
CCS improvement is less about “learning more medicine” and more about building a repeatable, time-safe workflow.
Below is a two-week plan you can run with any simulator. The plan assumes you can do 1–3 cases/day; adjust up or
down without changing the structure: timed reps + debrief + targeted redo.
If you want this plan auto-generated around your calendar and then adjusted based on your misses, MDSteps’ platform
can build an automatic study plan and track your case-level patterns, so your practice time targets the errors that
actually cost points.
Test-day CCS is a performance task. Your goal is to look like a competent, unsupervised generalist: stabilize,
diagnose, treat, monitor, and safely disposition. The biggest point losses come from (1) late critical therapy,
(2) wrong setting, (3) missing monitoring/reassessment, and (4) wasteful over-ordering. Use the checklist below
to make your performance consistent across every case, including the weird ones.
Most learners don’t need three simulators. They need one simulator that builds the right habits, the official
cases for calibration, and a plan that forces deliberate improvement. If your main weakness is software
fluency and exposure, prioritize a large case bank. If your weakness is timing, monitoring, or
disposition, prioritize physiology-driven reps and debriefs that tell you exactly what to change.
Want physiology-driven CCS practice with timed orders and a scorecard that shows exactly what you missed and how to fix it?
Try MDSteps’ Step 3 CCS cases alongside your QBank and run the 14-day plan above.
Compare the best Step 3 CCS cases platform—MDSteps, CCSCases.com, UWorld, and others—ranked by realism, feedback, and test-day transfer, plus a training plan.
Practice 135 CCS cases plus Step 3 QBank for $27/month.
Why your CCS simulator choice matters more than your case count
What CCS is actually testing
What CCS platforms should train (but many don’t)
A practical ranking rubric: the 6 features that predict test-day transfer
Rubric domain
What “excellent” looks like
Why it matters on Step 3
Interface fidelity
Free-text ordering, realistic chart layout, clock controls, and case-end behavior that feels like Primum.
Reduces cognitive load so you can focus on management rather than software navigation.
Physiology realism
Vitals/labs respond plausibly to interventions and time; wrong moves create believable deterioration.
Forces “treat → reassess → advance time” loops that match CCS scoring logic.
Scoring transparency
Clear breakdown of points: diagnosis, therapy, monitoring, timing/sequence, and setting.
Lets you fix the true problem (eg, correct order but late; correct treatment but wrong setting).
Debrief actionability
Shows missed high-yield orders, harmful/unnecessary actions, and a better sequence you can rehearse.
Turns each case into a repeatable algorithm instead of a one-off “gotcha.”
Case breadth + curation
Core emergencies + ambulatory care + inpatient management; minimal redundancy.
Prevents overfitting to a narrow pattern set; Step 3 mixes settings and acuity.
Workflow + analytics
Tracks trends across cases (missed monitoring, late antibiotics, wrong disposition) and drills weaknesses.
CCS improvement is pattern-based; you win by eliminating recurring “silent” errors.
How to use this rubric (fast)
Common CCS weaknesses the rubric will reveal
Compare less. Start practicing for less.
A simpler way to start practicing today.
See how it works
Ranked comparison: major CCS simulators side-by-side
Rank*
Platform
Best for
Strengths
Limitations
Quick pick
#1
MDSteps
Students who need physiology-driven practice + analytics to fix repeat mistakes.
Live vitals/labs responses, timed orders, outcome-based scoring, robust scorecards and trends.
Smaller ecosystem than legacy tools; best value when used with a structured plan.
If you miss points on timing/monitoring/disposition, start here.
#2
CCSCases.com
High-volume repetition to build interface fluency and a broad order vocabulary.
Large case bank, realistic feel, large order database, end-of-case grading/feedback.
Physiology depth varies by case; analytics are more case-by-case than longitudinal.
Great “mileage” if you can grind many cases quickly.
#3
UWorld CCS
UWorld users who want CCS familiarity inside one subscription and strong explanations.
Free-text order entry emphasis; educational explanations; integrates with Step 3 QBank workflow.
Time-cost can be high; feedback may feel less granular for sequencing errors.
Solid all-in-one if you already live in UWorld.
#4
MasterCCS
Learners who want real-time scoring cues while working through cases.
Emphasizes real-time scoring and detailed feedback; broad order database.
Less “battle-tested” by large user base vs CCSCases/UWorld; verify case breadth and updates.
Consider as a supplemental “feedback-first” option.
Baseline
USMLE sample CCS
Everyone, regardless of platform.
Official Primum feel; calibrates your expectations for case flow and clock behavior.
Limited number of cases; not enough alone for skill building.
Do these early, then again in the final week.
Not a simulator
AMBOSS
QBank + knowledge gaps (Step 3 MCQ), not CCS simulation.
Strong library and question bank workflows.
Does not provide Step 3 CCS simulations (as of current public statements).
Use for MCQ; pair with a CCS simulator.
Deep dive: what each platform does well (and where it can cost you points)
High-yield habits it reinforces
Where you still need to be intentional
Strengths that translate
Watch-outs
Strengths that translate
Watch-outs
How to choose based on your timeline: 4 common purchase scenarios
Scenario A: 10–14 days left, minimal prep time (intern schedule)
Scenario B: 3–6 weeks, solid knowledge but CCS anxiety
Scenario C: IMG or away from clinical care
Scenario D: Strong CCS, weak Step 3 MCQ
A 14-day CCS training plan that actually improves your score
Days
Primary objective
Daily case work
Debrief focus
1–2
Interface calibration + baseline habits
Official sample cases + 1 timed simulator case
Where did you lose time? What buttons/searches slowed you down?
3–5
Emergency workflow (ABCs, disposition)
2 timed ED cases/day (sepsis, chest pain, SOB, altered mental status)
Did life-saving therapy happen first? Were you in the right setting?
6–8
Inpatient management + monitoring
2 timed inpatient cases/day (CHF, DKA/HHS, GI bleed, pancreatitis)
Missing telemetry? repeat vitals? strict I/Os? DVT prophylaxis?
9–11
Clinic logic + preventive care
2 timed clinic cases/day (DM, HTN, prenatal, outpatient infections)
Follow-up intervals, counseling, vaccines/screening where relevant
12–13
Mixed settings + time stress
3 timed cases/day; force yourself to finish with 2 minutes spare
Identify top 3 recurring mistakes and write “if-then” fixes
14
Final calibration + confidence
Redo official cases + 1–2 “weakness” cases
Run your checklist; practice calm pacing and close-out orders
Your default CCS sequence (memorize this)
How to debrief in 4 minutes (no fluff)
Exam-day essentials: closing orders, time traps, and what not to do
Rapid-Review Checklist (printable)
High-yield “don’t do this” list
Bottom line recommendations and how to combine platforms efficiently
If you can only pick one
A simple combo that works
One-sentence CTA (keep it simple)
Citations & external references
CCS Cases
Best Step 3 CCS Cases Platforms in 2026: MDSteps vs CCSCases vs UWorld
USMLE Step 3
CCS strategy
Updated: Feb 8, 2026
What you’ll get
MDSteps Step 3 CCS Practice
Board-style trap: CCS punishes “smart-looking” over-ordering.
The higher your anxiety, the more likely you are to reflexively order broad panels and unnecessary imaging.
A strong simulator doesn’t just show what to order—it trains restraint and sequencing.
Full access: $27/mo
Lifetime: $299
16,000+ questions$27/month full accessCancel anytime
Monthly access. Cancel anytime. No free trial required.
Lower-friction QBank
Rule: spend ≤5 minutes reviewing the debrief, then immediately do another case that targets the same weakness.
Your target outcome is not “high percentage” early. It’s a steep improvement curve by week two.
Make a one-page template: ED stabilizers, inpatient maintenance orders, discharge/follow-up checklist.
CCS is a quarter-ish of the exam experience; you still need enough MCQ points to buffer tough cases.
Time trap to anticipate: if you place orders but don’t advance the clock to the report time,
you won’t see results or treatment effects. Conversely, if you advance time with no pending results, the case
may jump forward unexpectedly. Plan your clock moves.
Medically reviewed by: Jennifer L. Nguyen, MD