Start With the Real Question Behind UWorld Passes
Students often ask how many UWorld passes are needed for Step 2 CK because they want a simple rule that lowers uncertainty.
Students often ask how many UWorld passes are needed for Step 2 CK because they want a simple rule that lowers uncertainty. The better question is more diagnostic: what type of learning is your current pass producing? A complete first pass can be enough for a strong score when it is done in timed, mixed blocks, reviewed carefully, and followed by objective improvement on NBME or UWSA style assessments. A second full pass can help some students, but it can also become a false signal if the student remembers question stems without fixing the reasoning error that caused the miss.
Step 2 CK is a clinical decision-making exam. The official exam description emphasizes applying medical knowledge and clinical science to patient care under supervision, including diagnosis, management, health maintenance, and disease prevention. That matters because the exam rewards transfer. You are not only being asked whether you saw a fact in an explanation. You are being asked whether you can recognize a clinical pattern, choose the next best step, avoid a tempting distractor, and manage uncertainty under time pressure.
A UWorld pass is useful only if it builds those behaviors. A passive first pass, in which the student reads explanations but does not classify errors, often leads to the common complaint: “I finished UWorld and still do not feel ready.” By contrast, an active first pass can produce major gains because each block becomes a rehearsal of board-style reasoning. The student identifies why an answer was tempting, what clue should have redirected the diagnosis, and what rule will prevent the same miss next time.
For most Step 2 CK examinees, the highest-yield sequence is a full first pass plus structured review of incorrects and weak systems. A second complete pass is most useful when the first pass occurred during clerkships over many months, when retention is poor, or when the student’s NBME scores remain below the target range after incorrects. It is less useful when the student is close to exam day and has not yet done enough self-assessment review, CMS forms, or timed mixed blocks.
Minimum effective plan
One complete pass, incorrects, marked questions, and NBME-guided review.
Second pass helps when
The first pass was old, fragmented, or too passive to build recall.
Second pass hurts when
It replaces fresh assessment, CMS forms, or deliberate review of mistakes.
The goal is not to finish a resource twice. The goal is to reach a point where your performance is reproducible on new questions. That is why a student with a thoughtful first pass and rising NBMEs may not need a full repeat, while a student with two superficial passes may still be unsafe. Count passes only after you define what each pass is supposed to accomplish.
What a High-Quality First Pass Should Look Like
A high-quality first pass is not simply completion.
A high-quality first pass is not simply completion. It is a system for learning the clinical grammar of Step 2 CK. The best default is timed, mixed mode once you have enough baseline knowledge to tolerate it. Tutor mode can be reasonable early in a clerkship or during a weak subject rebuild, but dedicated Step 2 CK preparation should progressively resemble exam conditions. Timed mixed blocks force interleaving, which is closer to the real exam than doing all cardiology, then all obstetrics, then all pediatrics.
Review should be slower than answering. A common mistake is spending one hour on a 40-question block and only 30 minutes reviewing it. For most students, the value is in the review. Each missed question should be labeled by error type: knowledge gap, misread clue, wrong illness script, premature closure, management sequencing error, or test-taking trap. This classification changes the next action. A knowledge gap may need a flashcard. A management sequencing miss may need a mini-algorithm. A misread clue may need a timing or highlighting adjustment.
Correct questions deserve review too. If you guessed correctly, eliminated poorly, or selected the right answer for the wrong reason, that question is not truly mastered. Many Step 2 CK plateaus come from counting lucky corrects as learned material. During review, ask three questions: what finding made the right answer best, why was the strongest distractor wrong, and what would need to change in the stem to make that distractor correct?
The first pass should also generate an organized review product. This does not mean copying paragraphs. It means extracting rules. A useful note sounds like: “Pregnant patient with hypertension after 20 weeks plus thrombocytopenia or elevated liver enzymes suggests preeclampsia with severe features, so management depends on stability and gestational age.” A weak note sounds like: “Read preeclampsia.” The first note changes future behavior. The second only records guilt.
| Finding During Review | Likely Problem | Best Fix |
|---|---|---|
| Missed a classic presentation | Weak illness script | Create a two-line pattern card with key clues and next step. |
| Changed from right to wrong | Poor confidence calibration | Write why the original answer was supported and what triggered doubt. |
| Picked diagnosis when asked management | Question stem task error | Underline the final sentence before reading answer choices. |
| Missed because of outdated memory | Stale clinical rule | Update the rule from a trusted reference and practice similar questions. |
| Ran out of time | Inefficient block pacing | Use 10-question checkpoints and practice moving on from low-yield uncertainty. |
This is where a platform can be useful when it reduces friction rather than adding another resource. MDSteps can support this workflow through an Adaptive QBank, automatic flashcard decks from missed questions that can be exported to Anki, and an exam readiness dashboard that keeps weak systems visible. The key is still the behavior: every question should produce either confidence, correction, or a plan.
When One Pass Is Enough
One complete UWorld pass may be enough when three conditions are met.
One complete UWorld pass may be enough when three conditions are met. First, your first pass was active and recent. Second, your practice scores are near or above your target. Third, your misses are becoming narrower and more predictable. In this setting, a full second pass may deliver diminishing returns because many questions will feel familiar. Familiarity can create a dangerous sense of mastery. Step 2 CK does not test whether you recognize an old explanation. It tests whether you can solve a new vignette with the same principle.
A strong one-pass student usually shows a pattern. Early blocks are uneven, then timed mixed performance rises, then NBME scores confirm improvement on new items. Review logs show fewer broad content gaps and more isolated misses. The student can explain why common distractors are wrong. For example, they do not only know that acute cholecystitis presents with right upper quadrant pain. They know when ultrasound is preferred, when HIDA is considered, when antibiotics are needed, and how cholangitis changes urgency.
For these students, the next step after finishing UWorld is not automatically a second pass. It is targeted consolidation. That may include incorrects, marked questions, CMS forms in weak clerkship areas, NBME self-assessments, and focused review of preventive care, ethics, quality improvement, biostatistics, and common management algorithms. The final weeks should be spent increasing transfer to new questions, not proving that you remember old ones.
One pass is also more likely to be enough if UWorld was integrated with clerkships. Students who used questions during pediatrics, surgery, medicine, psychiatry, obstetrics and gynecology, and family medicine often build a longitudinal foundation. If they continued reviewing old misses and used self-assessments during dedicated, they may not need to redo every question. Their challenge is often integration. They need mixed blocks and broad NBME review to shift from shelf mode to Step 2 CK mode.
A one-pass plan is not a shortcut. It is a quality threshold. The student still needs enough question volume to encounter common presentations, enough review to repair errors, and enough self-assessment data to confirm readiness. The number of passes becomes less important than the evidence that your reasoning holds up on unfamiliar stems.
When a Second Pass Is Worth It
A second pass is worth considering when the first pass did not function as dedicated Step 2 CK preparation.
A second pass is worth considering when the first pass did not function as dedicated Step 2 CK preparation. This is common. Many students start UWorld during clerkships, spread questions over a year, and finish with large gaps between early blocks and test day. In that case, “one pass complete” may overstate readiness. The early medicine, surgery, or pediatrics questions may be functionally new again. A second exposure can be useful if it is selective, timed, and error-driven.
The second pass should not be a mechanical reset. It should answer specific questions: Do you still miss the same diagnoses? Do you still choose the wrong next best step? Do you still confuse similar presentations? Are you too slow in mixed blocks? If the answer is yes, a repeat can help, but only if you review differently from the first time. Redoing the same explanations in the same passive way usually reproduces the same score plateau.
A full second pass is most appropriate for students with a longer runway, usually six or more weeks, especially if their baseline is far from the target. Students with three weeks or less often get more value from incorrects, NBME review, CMS forms, and focused content repair. Time matters because a second pass can consume hundreds of hours. That investment must compete against other high-yield activities.
The biggest benefit of a second pass is retrieval practice. You are asking your brain to reconstruct the reasoning pathway. The biggest risk is recognition memory. If you remember the answer from the stem, you may score well without improving. To reduce that risk, force yourself to verbalize the rule before selecting. For every repeated question, say: “The key clue is X, the diagnosis or task is Y, and the reason the answer is Z.” If you cannot do that, the question is still useful. If you can only remember that the answer was option C, it is not.
More than several months ago
NBME trend not reassuring
Timed, mixed, error-labeled
A selective second pass often beats a full second pass. Start with incorrects and marked questions. Then add weak systems based on your analytics and self-assessments. If medicine management, obstetric triage, pediatric infections, or surgery complications are repeatedly weak, redo those categories in mixed sets with related disciplines. The aim is not aesthetic completion. The aim is score movement on new questions.
Use NBME Scores to Decide, Not Pass Count Alone
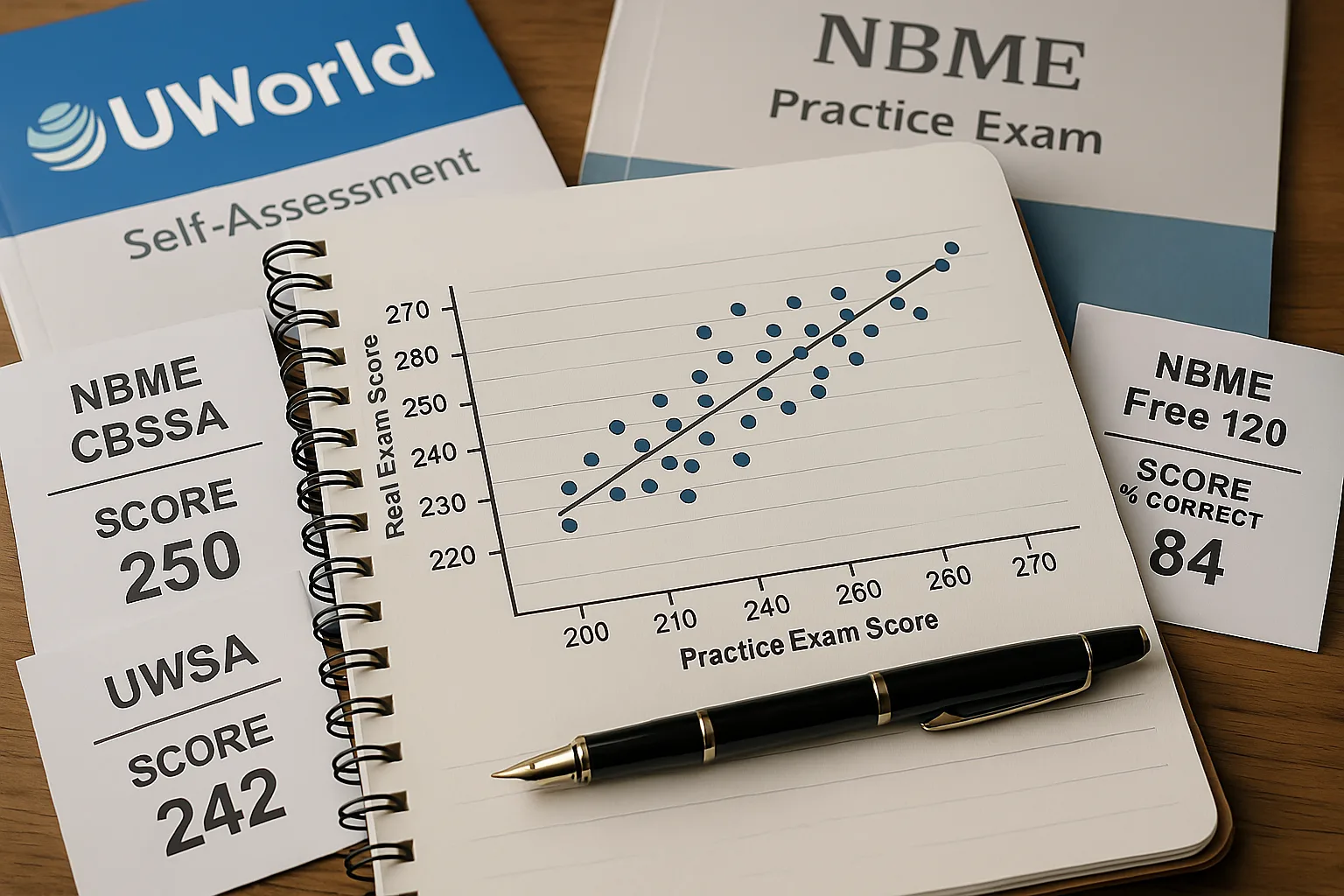
NBME self-assessments are useful because they test transfer.
NBME self-assessments are useful because they test transfer. UWorld is a learning resource. NBME-style self-assessments help determine whether that learning is converting into exam performance. A student who completes two UWorld passes but has stagnant NBME scores needs a diagnostic change, not more completion. A student who completes one pass and shows a steady NBME rise may be using the resource correctly.
After each self-assessment, review missed questions by category. Separate content misses from reasoning misses. A content miss means you did not know the disease, test, treatment, screening recommendation, or complication. A reasoning miss means you knew the topic but failed to apply it. Step 2 CK students often overestimate content gaps and underestimate reasoning gaps. They respond by reading more when they should be practicing task recognition, next-step sequencing, and distractor control.
The timing of self-assessments matters. A baseline can be taken early to identify the gap. Midpoint assessments should guide whether to continue broad UWorld completion or shift into weak-area repair. Final assessments should confirm readiness under timed conditions. Do not take an NBME, look only at the score, and move on. The score is the headline. The misses are the curriculum.
Use a simple decision rule. If scores are rising and approaching your target, continue the plan and avoid panic switching. If scores are flat despite high question volume, change how you review. If scores fall after finishing a pass, consider fatigue, poor retention, too much recognition-based studying, or neglect of NBME-style logic. The answer may be targeted review, not another full resource cycle.
| Your Situation | Best Next Move | Avoid |
|---|---|---|
| NBME scores at or above goal | Incorrects, marked items, CMS forms, and final weak-topic review. | Resetting everything out of anxiety. |
| Scores improving but still below goal | Targeted second pass in weak systems plus self-assessment review. | Only reading notes without timed practice. |
| Scores stagnant after many blocks | Error audit, reasoning drills, and a new review method. | More question volume with the same passive review. |
| Scores inconsistent | Analyze pacing, fatigue, careless misses, and mixed-block endurance. | Assuming all variability is content weakness. |
MDSteps can help here when the analytics identify whether the problem is system-based, task-based, or caused by repeated misses from the same clinical pattern. For Step 2 CK, consider pairing the Step 2 CK study tools with careful self-assessment review so your plan is driven by evidence rather than fear.
How to Review Incorrects Without Memorizing Answers
Incorrects are often the highest-yield part of UWorld, but only when they are reviewed as patterns.
Incorrects are often the highest-yield part of UWorld, but only when they are reviewed as patterns. The trap is to redo incorrects too soon and celebrate a high percentage. That may only mean you remembered the question. Space the review when possible. When you return to an incorrect, cover the answer choices and force yourself to name the diagnosis, the task, and the next step. Then look at the choices. This converts a repeated question into retrieval practice instead of recognition practice.
A strong incorrect review has four outputs. First, a corrected illness script. Second, a next-step rule. Third, a distractor contrast. Fourth, a prevention plan. For example, if you missed pulmonary embolism in pregnancy, the output should not be “review PE.” It should identify the stem clues, the safest diagnostic sequence, the role of imaging, and the reason another option was less appropriate. You are building a rule that can survive a new vignette.
Marked questions should be handled similarly. Mark a question if it exposes uncertainty, not simply because it was difficult. If every hard question is marked, the list becomes unusable. A good marked list contains questions that represent recurring traps: renal failure changing drug selection, pregnancy changing imaging choices, postoperative fever timing, pediatric dehydration severity, or psychiatric safety assessment. These are the questions that often recur conceptually on Step 2 CK.
Flashcards can help, but they should be concise and clinical. Avoid long cards that reproduce explanations. Use cards for rules, thresholds, discriminating clues, and management sequences. A good card asks: “Postpartum patient with severe headache, hypertension, and visual symptoms: what diagnosis and next management priority?” A poor card asks: “What is preeclampsia?” The exam rarely rewards isolated definitions. It rewards application.
When reviewing incorrects, also track repeated distractors. If you often choose antibiotics when the correct answer is drainage, imaging when the correct answer is stabilization, or reassurance when the correct answer is urgent evaluation, you have a management sequencing issue. That deserves a checklist or algorithm, not another paragraph of reading. Step 2 CK repeatedly tests the order of action: stabilize first, identify emergencies, choose the most appropriate diagnostic test, and treat based on severity.
Incorrect Review Template
- Clue: What detail should have changed your answer?
- Task: Was the question asking diagnosis, next step, treatment, screening, or complication?
- Trap: Which answer was attractive but wrong, and why?
- Rule: What one-sentence principle will prevent the miss?
- Recheck: When will you test the rule again?
The best incorrect review is uncomfortable because it exposes why you missed the question. That is the point. A second pass is valuable only if it makes those errors visible and correctable.
Build a Pass Strategy Around Your Timeline
Your timeline should determine how aggressively you pursue another pass.
Your timeline should determine how aggressively you pursue another pass. A student with twelve weeks can use a broad first pass, targeted content repair, incorrects, and several self-assessments. A student with four weeks must be more selective. A student with two weeks should not reset a large question bank unless the reset is part of a focused plan. The closer you are to exam day, the more every hour must compete against NBME review, CMS forms, weak-topic algorithms, sleep, and endurance.
For eight to twelve weeks, a full first pass is realistic if you can complete consistent daily blocks. Start with system-based support only if your foundation is weak, then move into timed mixed blocks. Use one day per week for catch-up, self-assessment review, or weak areas. After completion, redo incorrects and marked questions. Add CMS forms for clerkship-style weak points and NBME assessments to confirm transfer.
For four to six weeks, do not chase perfection. Prioritize timed mixed UWorld blocks, incorrect review, and NBME-driven weak areas. If you have already completed most of UWorld, do not assume that a full second pass is required. Use incorrects first. Then sample weak systems. If you have not completed UWorld, finish the highest-yield remaining blocks while preserving time for assessment review. A rushed first pass with no review is less valuable than a slightly smaller volume done well.
For two to three weeks, the plan becomes surgical. Review recent NBMEs, redo incorrects in the weakest systems, practice timed mixed blocks, and cover high-frequency areas such as ethics, quality improvement, preventive care, biostatistics, obstetric triage, emergency presentations, and common medicine management. This is not the time to create a new giant note system. It is the time to stabilize performance and reduce repeat errors.
| Time Until Exam | UWorld Priority | Assessment Priority | Main Risk |
|---|---|---|---|
| 8 to 12 weeks | Complete first pass, then incorrects and marked questions. | Baseline, midpoint, and final NBME or UWSA sequence. | Moving too slowly through review. |
| 4 to 6 weeks | Finish high-yield blocks or targeted second pass. | Use each assessment to choose the next week’s focus. | Trying to redo everything without enough review. |
| 2 to 3 weeks | Incorrects, weak systems, timed mixed sets. | Final readiness confirmation and detailed miss review. | Resource switching and anxiety-driven resets. |
Students who are unsure how to allocate time should use an automatic study plan generator or structured calendar. The schedule should be realistic enough to follow when tired. A plan that assumes ten perfect hours every day often collapses by day four. The best plan protects review time, sleep, and self-assessment analysis because those are the activities that make question volume productive.
Rapid-Review Checklist for Deciding on Another Pass
Before committing to another full UWorld pass, run a readiness audit.
Before committing to another full UWorld pass, run a readiness audit. The purpose is to decide whether a second pass is the best use of time or whether a targeted plan would produce more score movement. Be honest. Many students do not need another pass. They need better review, more new-question transfer, and tighter management algorithms. Other students do need a second exposure because the first pass was too old, too fragmented, or too passive.
Exam-Day Essentials and Pass Decision Checklist
- I completed most or all of a first pass with active review, not just reading explanations.
- I can explain my most common error types without vague language.
- My NBME or UWSA trend is improving or clearly identifies weak areas.
- I have reviewed incorrects after enough spacing to test recall.
- I can answer timed mixed blocks without major pacing collapse.
- I have a plan for ethics, quality improvement, biostatistics, prevention, and screening.
- I know which systems still cost points and how I will repair them.
- I am not using a second pass to avoid taking or reviewing self-assessments.
If most items are checked and your scores are near your target, a full second pass is probably not mandatory. Use the remaining time for incorrects, marked questions, assessment review, and weak-topic refinement. If several items are unchecked, decide why. If the issue is poor recall from an old first pass, a targeted repeat may help. If the issue is reasoning, pacing, or careless reading, a second pass will only help if it is paired with specific behavior changes.
The most practical answer is this: one excellent pass can be enough, one passive pass is rarely enough, and two passive passes are still not a strategy. Step 2 CK preparation should be measured by your ability to solve new clinical vignettes, not by the number of times a question bank dashboard says complete. Use UWorld as a training tool, NBMEs as transfer checks, and your error log as the bridge between the two.
For a broader framework on dissecting clinical vignettes, review the MDSteps sample question breakdown. A disciplined question review process can turn every missed item into a durable rule, which is the real purpose of any pass through a question bank.
Daniel R. Menendez, MD, Internal Medicine.
References
- United States Medical Licensing Examination. Step 2 CK Content Outline and Specifications. Accessed May 27, 2026. https://www.usmle.org/exam-resources/step-2-ck-materials/step-2-ck-content-outline-specifications
- United States Medical Licensing Examination. Step 2 CK Materials. Accessed May 27, 2026. https://www.usmle.org/exam-resources/step-2-ck-materials
- National Board of Medical Examiners. Comprehensive Clinical Science Self-Assessment. Accessed May 27, 2026. https://www.nbme.org/examinees/self-assessments/comprehensive-clinical-science-self-assessment
- United States Medical Licensing Examination. Step 2 CK Sample Test Questions. Accessed May 27, 2026. https://www.usmle.org/exam-resources/step-2-ck-materials/step-2-ck-sample-test-questions
- Serra MJ, et al. The use of retrieval practice in the health professions. Perspect Med Educ. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12292765/
- Thompson CP, et al. The effectiveness of spaced learning, interleaving, and retrieval practice in health professions education. J Am Coll Radiol. 2023. https://www.jacr.org/article/S1546-1440(23)00646-4/fulltext
UWorld explains the medicine. MDSteps explains the decision.
Traditional review often tells you the correct answer. MDSteps helps isolate the decision error: the missed pivot clue, the tempting distractor, the timing mistake, or the weak rule that failed under pressure.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.