At its heart, differential diagnosis is structured reasoning under pressure. Step 2 CK questions are crafted to test how efficiently you can connect clinical clues, filter noise, and recognize probability. The key is not memorizing every disease but building frameworks: symptom clusters, timing, and demographic anchors. For example, chest pain can be organized by mechanism—ischemic, inflammatory, pleuritic, or psychogenic—each tied to distinct risk patterns and exam cues. High-yield test writers often design distractors that mimic real-world overlap: pericarditis versus myocardial infarction, or Crohn’s versus ulcerative colitis. Differentiating comes down to weighted clues—position relief, lab trends, chronicity, and associated findings. Practicing structured comparisons builds the speed and accuracy expected on exam day. Within MDSteps, each QBank question tags reasoning domains (“localization,” “pattern recognition,” “probability weighting”), allowing you to analyze which diagnostic logic pathways you favor or neglect. Over time, this data guides targeted remediation, improving both accuracy and timing. Building differentials begins with categorization. Instead of memorizing conditions, learn to assign symptoms into system-based algorithms—neurologic, cardiopulmonary, endocrine, or infectious. When presented with a symptom, train your mind to ask: “Which systems can explain this?” Then, move from broad to narrow, using exclusion logic and diagnostic probabilities. Practice creating similar tables from question sets. MDSteps’ analytics allow exporting missed topics into Anki decks, ensuring spaced reinforcement of weak diagnostic links. Effective diagnostic reasoning relies on “weighted clues”—some findings carry more discriminatory value than others. For instance, pulsus paradoxus in cardiac tamponade outweighs nonspecific chest pressure. On Step 2 CK, recognize which clues anchor a disease pattern and which are distractors. Train yourself to mentally assign weight scores: “high-yield clue,” “moderate clue,” “nonspecific clue.” Use MDSteps QBank filters to practice questions tagged as “pattern differentiation.” After reviewing each case, verbalize why competing diagnoses were less likely—this metacognitive step hardwires clinical logic and prevents premature closure. Train next-best-step reasoning with adaptive clinical blocks, 50/50 trap analysis, and targeted review recommendations. Many Step 2 CK questions require the skill of exclusion rather than confirmation. Strong differential builders think probabilistically: “What is most consistent? What is least plausible?” Apply Bayesian reasoning intuitively by contrasting the probability of each diagnosis given the clues. Avoid emotional elimination (“I don’t remember that condition”) and rely instead on logic (“this disease wouldn’t cause bilateral findings”). During practice, use MDSteps’ rationales to trace how distractors are constructed. Recognizing their pattern—misapplied lab values, similar imaging, overlapping demographics—helps dismantle them quickly on test day. To internalize differential reasoning, blend it into every part of your study cycle. When reviewing a missed question, don’t just note the right answer—build a mini flowchart for how to reason toward it. MDSteps’ auto-generated flashcards from your misses can include “next-step” reasoning prompts, forcing you to reconstruct your diagnostic pathway later. With repetition, pattern recognition becomes instinctive, not forced—a hallmark of advanced Step 2 CK test-takers. Step 2 CK rewards clarity over speed. Average high-scorers spend ~75 seconds per question, balancing interpretation and elimination. On exam day, triage questions: read the final line first (“What is the most likely diagnosis?”), then scan for pathognomonic or exclusionary clues. Mark uncertain items but keep moving—your diagnostic frameworks will subconsciously process during later blocks. Before test day, use MDSteps’ full-length simulations and readiness dashboard to identify pacing gaps and reasoning slowdowns. Reviewing your diagnostic accuracy curve (accuracy ÷ time ratio) gives quantitative insight into reasoning efficiency—a critical Step 2 CK skill. Combat these by deliberate reflection: ask, “What else could this be?” before locking in an answer. MDSteps’ QBank feedback prompts this metacognitive step after each question, reinforcing open diagnostic reasoning. Consistent use of structured reasoning turns uncertainty into a process—and process into points. By exam day, you won’t just recognize diseases; you’ll understand how the test thinks. Developing expert-level differential diagnosis skills continues beyond Step 2 CK. Use every clinical rotation to reinforce diagnostic reasoning: predict likely causes before preceptor feedback. MDSteps’ adaptive analytics continue to refine this skill set, showing real-time progress toward diagnostic mastery. Whether in questions, wards, or residency, the habit of structured reasoning remains your strongest clinical asset.
References & Further Reading:The Core of Differential Diagnosis on Step 2 CK
From Symptoms to Systems: Creating Diagnostic Frameworks
Symptom
Top Differential Categories
Key Discriminators
Fever + Rash
Infectious, Autoimmune, Drug Reaction
Timing, Distribution, Mucosal involvement
Chest Pain
Cardiac, Pulmonary, GI, Musculoskeletal
Onset, Exertion link, Positional change
Abdominal Pain
Visceral, Parietal, Referred, Functional
Location, Guarding, Temporal pattern
Pattern Recognition and the “Weighted Clue” Approach
Turn this into Step 2 decision practice
Stop picking between two good-sounding answers.
See how it works
Elimination Logic: Ruling Out with Purpose
Integrating Diagnostic Skills into Study Workflow
Exam-Day Reasoning and Time Management
Common Pitfalls in Differential Diagnosis
Rapid-Review Checklist: Differential Diagnosis Mastery
Next Steps and Continued Growth
1. NEJM — Diagnostic Reasoning Frameworks
2. Oxford Academic — Clinical Decision-Making Biases
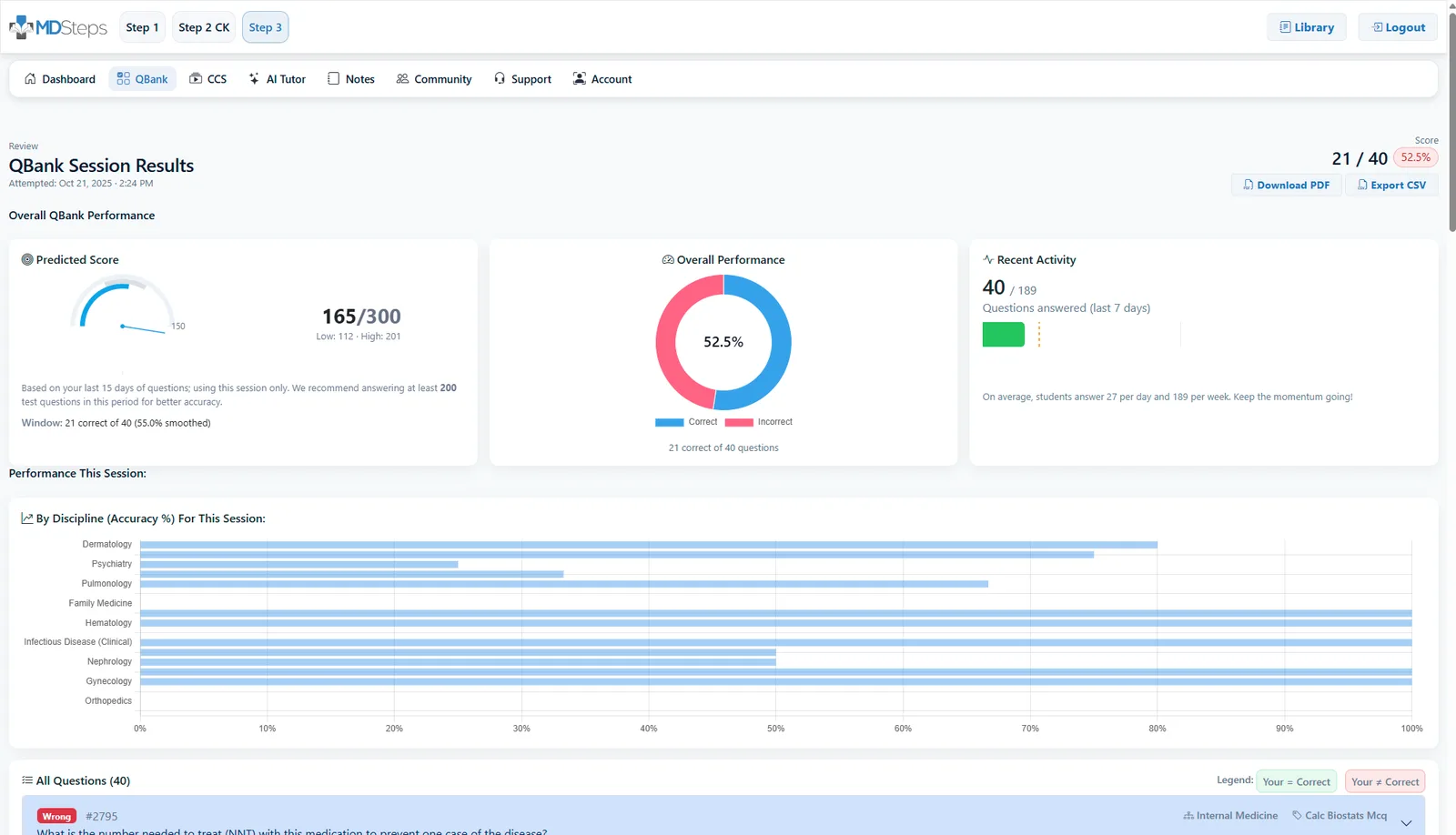
3. MDSteps Adaptive QBank & Analytics Dashboard
USMLE Step 2 CK
How to Build Differential Diagnosis Skills for Step 2 CK

Master differential diagnosis skills for Step 2 CK by understanding disease patterns, integrating pathophysiology with clinical clues, and practicing targeted reasoning using the MDSteps Adaptive QBank and analytics dashboard.
Full access: $27/mo
Lifetime: $299
Clinical decision blocks50/50 trap analysisWeak-area review
Monthly access. Cancel anytime. No free trial required.
Step 2 reasoning