Get 16,000+ USMLE-style questions, 135 CCS cases, stem decoding, visual rationales, analytics, flashcards, and reasoning-focused review in one subscription. Cancel anytime. First month protected by our 7-day good-faith refund guarantee after 100 questions or 5 CCS cases. The Step 2 CK practice exam correlation is one of the most analyzed topics among test-takers. Every student wants to know: “If I scored 250 on UWSA 2, what will I actually get on test day?” The answer depends on which self-assessment you use, how far you are from the real exam, and how you handle exam conditions. Understanding correlation helps you gauge readiness, refine study focus, and reduce anxiety born of uncertainty. Correlation measures how tightly practice scores predict real Step 2 CK performance. When correlation r is 0.9, it means 90 percent of your variance in the real score is explained by practice results — a remarkably strong link. However, these exams sample different question styles, timing stress, and cognitive load. So even highly predictive assessments have confidence intervals of ±5–10 points. In 2025, students use three main tools — the NBME CBSSAs, the UWorld Self-Assessments (UWSA 1 and 2), and the NBME Free 120 (formerly known as the Practice Form). Each serves a different diagnostic purpose. When interpreted correctly, they form a triangulated estimate of real-exam performance. The Comprehensive Basic Science Self-Assessments (CBSSA) for Step 2 CK are retired NBME forms made public or sold through official channels. These are closest in content and psychometric scaling to the actual exam, because they use identical item calibration and scoring models. Typical correlation coefficients (r) between CBSSA and Step 2 CK scores range from 0.82 to 0.88 — highly reliable when taken within 3–5 weeks of the exam. Because CBSSAs mirror the NBME’s scoring logic, they’re most useful for gauging readiness thresholds: ≥ 245 is generally associated with top-quartile performance, while ≤ 220 indicates knowledge gaps requiring immediate review. MDSteps’ Adaptive QBank integrates CBSSA-style questions with live analytics, allowing you to generate predictive curves similar to NBME scaling in real time. Review the concept, then drill similar MDSteps questions so the same NBME-style pattern does not cost you points again. UWSA 1 and 2 remain the most widely used Step 2 CK practice tests. Their strengths are realistic pacing, strong clinical reasoning coverage, and visually similar interface to the real exam. However, UWorld’s standard-setting differs from NBME scaling — scores are often 3–7 points higher than actual performance. In recent cohort analyses, UWSA 2 correlates at r ≈ 0.88 with real scores, while UWSA 1 correlates at r ≈ 0.80. Because UWSA 2 includes items with higher cognitive integration and updated clinical vignettes, its predictive value is now comparable to the CBSSA series. MDSteps mirrors this approach through its Adaptive QBank’s Performance Prediction Model, which automatically projects your expected Step 2 CK range based on difficulty level and time to exam. Students often find the MDSteps forecast within ±4 points of actual NBME results. The NBME Free 120 (formerly the “Free Practice Exam”) is released annually with questions retired from Step 2 CK. It has no official scaling but is excellent for familiarity and pattern recognition. Recent analysis shows that percentage scores on the Free 120 roughly correlate as follows: Because the Free 120 is shorter and untimed, students often score higher than they would under real conditions. Nevertheless, it serves as an excellent pre-exam warm-up or day-before confidence booster. MDSteps includes a timed “NBME-style mode” that simulates the Free 120 interface with automated percentile conversion to a Step-scaled estimate. Because no single test perfectly predicts your Step 2 CK performance, the most accurate approach is to average recent scores weighted by predictive value. A simple formula used by many MDSteps students: Weighted Composite Score = (0.4 × CBSSA Avg) + (0.4 × UWSA 2) + (0.2 × Free 120 Converted Score) Subtract 3 points if taken > 4 weeks before exam; add 2 points if all taken under timed conditions. For example, if your CBSSA average = 248, UWSA 2 = 252, and Free 120 = 83 % (≈ 242), then Composite = 0.4(248) + 0.4(252) + 0.2(242) = 248.4 ≈ 248. This weighted score usually predicts final results within ±5 points. MDSteps’ dashboard does this automatically, plotting a real-time prediction curve so you can see trajectory improvement week by week. Students often face conflicting signals — for example, a UWSA 2 score of 256 but a CBSSA 11 of 240. Discordance is normal and reflects test variance, not sudden knowledge loss. Consider these factors: Use the lower score as your working baseline, then verify by taking a different assessment after 7–10 days. Avoid over-testing within the final week; score stabilization is more predictive than a single number. Spacing your practice exams intelligently prevents burnout and maximizes data accuracy. Below is a sample eight-week testing timeline used by top performers. MDSteps’ automatic study plan generator integrates this schedule with your QBank metrics so that you receive dynamic reminders when a new self-assessment is due. Each completed exam feeds into the Readiness Dashboard, which projects your expected Step 2 CK score on a confidence interval plot. Interpreting your Step 2 CK practice exam correlation is as much an art as a science. No practice test captures the exact stress, endurance, and novelty of exam day, but when your recent CBSSA and UWSA 2 scores converge within 5 points, you’re statistically ready. The MDSteps Adaptive QBank and Readiness Dashboard streamline this process, transforming raw data into confidence. Approach each practice exam as a diagnostic mirror, not a final verdict — and by test day, your data will speak for itself. References: USMLE Official Site | NBME Self-Assessment Portal | MDSteps PlatformStudy Step 1, Step 2 CK, Step 3, and CCS for $27/month.
Why Practice Exam Correlation Matters for Step 2 CK
CBSSA Forms: Still the Statistical Gold Standard
CBSSA Form Mean Overprediction (pts) Correlation (r) Best Testing Window Form 9 +2 to +4 0.84 5–6 weeks out Form 10 0 ± 5 0.86 3–5 weeks out Form 11 −2 to +1 0.87 ≤3 weeks out Turn your Free 120 misses into targeted practice
Do not just read why you missed it.
See how it works
UWorld Self-Assessments (UWSA 1 & 2): Realistic Timing, Slightly Inflated
NBME Free 120: Low-Stress, High-Yield Calibration
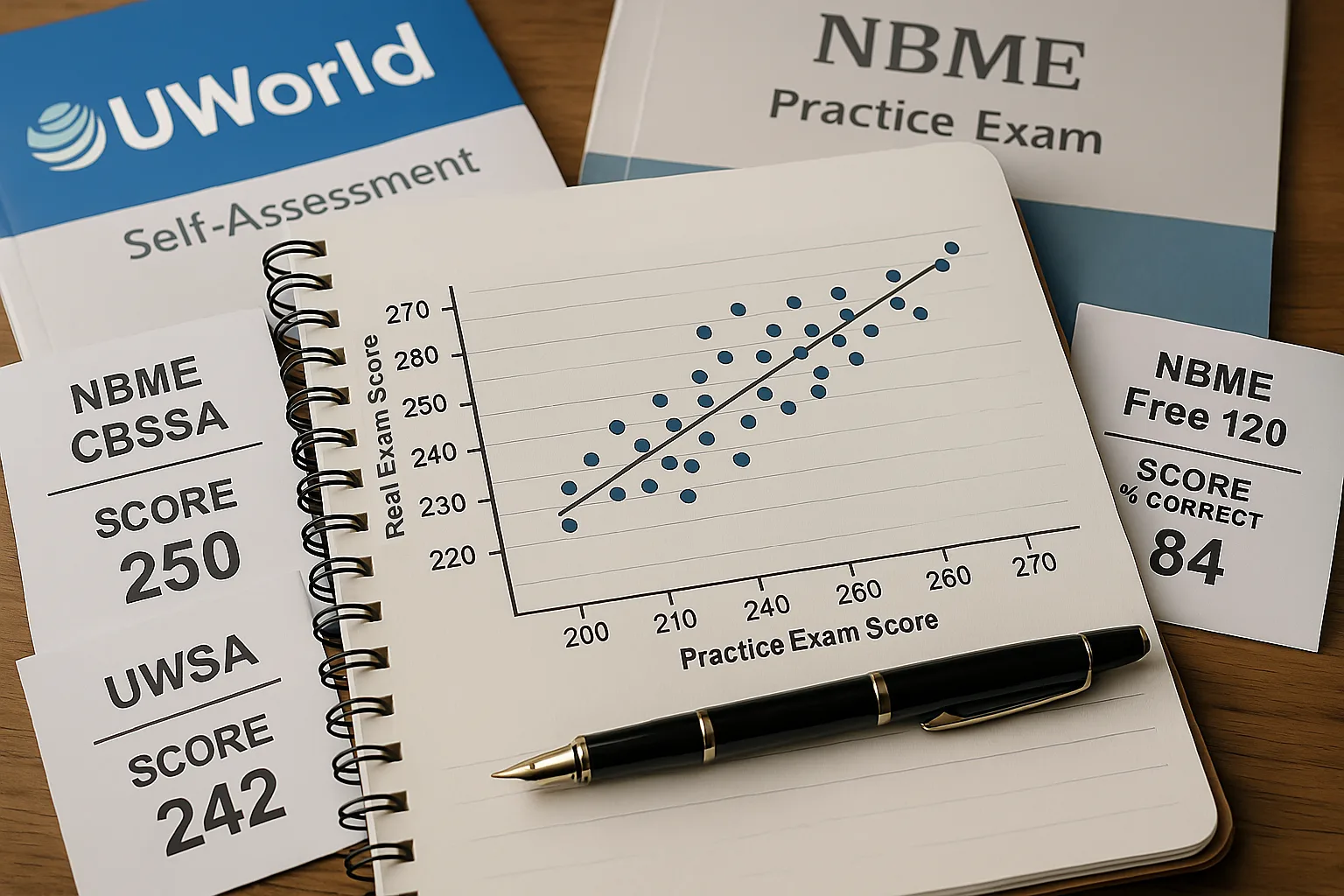
Free 120 % Correct Approx. Step 2 CK Score 90 % ≈ 260 + 85 % ≈ 250 80 % ≈ 240 75 % ≈ 230 70 % ≈ 220 How to Convert and Combine Multiple Practice Scores
Interpreting Discordant Scores
Practical Schedule for Self-Assessments
Week Assessment Purpose Week 8 CBSSA 9 Baseline diagnosis Week 6 UWSA 1 Adjust study plan Week 4 CBSSA 10 Confirm content mastery Week 3 UWSA 2 Full simulation under timed conditions Week 1 NBME Free 120 Final confidence check & interface practice Rapid-Review Checklist: Predicting and Improving Step 2 CK Scores
Final Thoughts: Data Confidence Before Exam Day
USMLE Step 2 CK
Step 2 CK Practice Scores vs Real Exam: NBME, UWSA, CBSSA, and Free 120
MDSteps Full Access
Full access: $27/mo
Lifetime: $299
NBME-style practice blocksWeak-topic reviewMissed-pattern analytics
Monthly access. Cancel anytime. No free trial required.
After the explanation