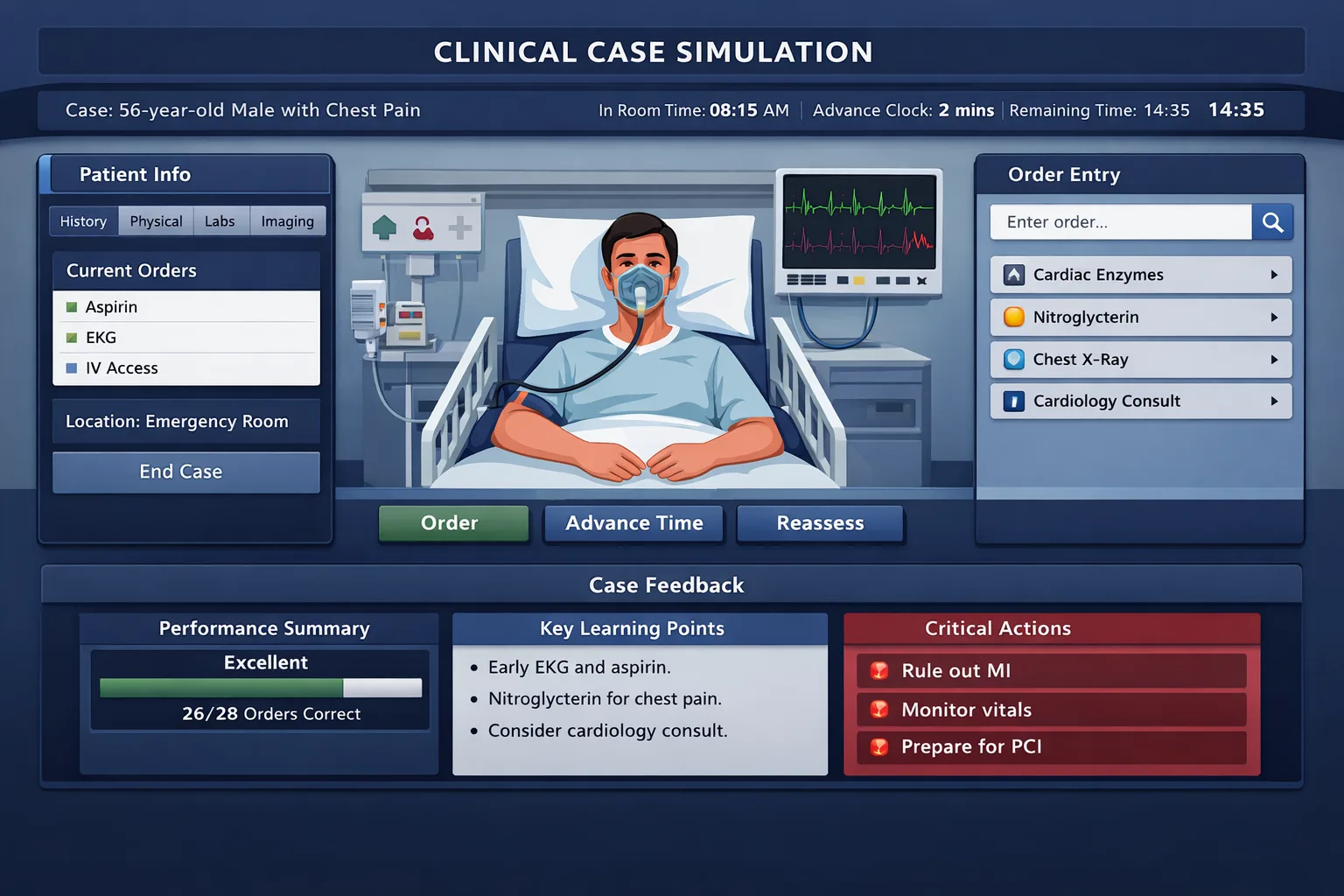
Step 3 CCS practice and initial orders require a safe, repeatable system for stabilizing patients, choosing focused diagnostics, starting treatment, and closing cases with prevention, counseling, and follow-up. Computer-based case simulations test more than diagnosis. They test whether a physician can manage a patient over time with safe prioritization. A multiple-choice question often rewards recognition of one best next step. CCS rewards sequence, timing, restraint, and completeness. The same diagnosis can score differently depending on whether the examinee stabilizes the patient before imaging, orders a pregnancy test before teratogenic therapy, monitors a toxic medication, or adds counseling before discharge. The official Step 3 format includes computer-based simulations on the second day. Cases may be short or longer, and each case requires the examinee to interact with the patient through orders, time advancement, reassessment, and disposition. The practical implication is simple: reading CCS explanations is not enough. Learners need deliberate practice in the software logic of placing orders, advancing time, and responding to interval updates. The central error many examinees make is treating CCS like a checklist of possible orders. That approach creates overtesting, delayed therapy, and missed safety steps. A better approach is to think in four linked questions: Is the patient unstable? What diagnosis or syndrome is most dangerous right now? What orders change outcome in the next few minutes? What orders complete long-term care once the acute problem is controlled? Recognize instability and place immediate safety orders before diagnostic delays. Order focused tests that confirm the leading diagnosis and exclude dangerous alternatives. Complete disposition, prevention, counseling, monitoring, and follow-up before the case closes. For preparation, the most useful cases are those that force action under time pressure. A good case bank should make the learner enter orders, watch simulated time move, and recognize when a stable outpatient differs from a septic inpatient. MDSteps fits this workflow by pairing a large Adaptive QBank with Step 3 CCS-style cases that use timed orders and live physiology. This matters because the exam does not simply ask what you know. It asks whether you can act safely with incomplete information. Initial orders should be driven by acuity, setting, and syndrome. A patient in the emergency department with hypotension, hypoxemia, chest pain, altered mental status, anaphylaxis, trauma, or sepsis needs immediate stabilization. A stable clinic patient with chronic fatigue, hypertension, diabetes follow-up, or preventive care does not need a reflexive hospital order set. CCS rewards appropriate care, not maximal care. Use an “ABC plus monitors” approach when the patient is unstable. Start with airway, breathing, circulation, mental status, and immediate monitoring. Pulse oximetry, cardiac monitor, blood pressure monitoring, intravenous access, oxygen when indicated, and isotonic fluids when appropriate are common safety orders. In parallel, choose tests that match the syndrome. Chest pain may need ECG, troponin, chest radiography, aspirin when appropriate, and anticoagulation or reperfusion logic depending on the presentation. Sepsis may need blood cultures, lactate, broad-spectrum antibiotics, fluids, and source evaluation. For stable patients, begin with targeted history and physical examination, then order focused diagnostics. Do not advance time after ordering only labs if a treatment should start immediately. Conversely, do not start definitive therapy without basic safeguards when the therapy has major risks. For example, pregnancy testing matters before many imaging and medication decisions. Renal function matters before nephrotoxic drugs or contrast. Coagulation status matters before invasive procedures or thrombolytic therapy. The best order set is neither sparse nor indiscriminate. It is justified by the patient’s immediate risk. A high-yield habit is to write a one-line working diagnosis before ordering: “This is likely unstable GI bleeding,” “This is outpatient diabetes follow-up,” or “This is possible ectopic pregnancy.” That sentence protects you from both undertreatment and overordering. Many learners complete cases passively. They read the prompt, glance at the answer, and assume they would have placed the correct orders. That method fails because CCS performance depends on execution. Practice should be active, timed, and reviewed in layers. Start each case by reading the location, age, sex, chief concern, vitals, and key history. Decide whether the case is emergent within 20 to 30 seconds. Then place only the first wave of orders. Pause before advancing time and ask: “Have I started any treatment that must not wait?” In an unstable patient, diagnostics and treatment often begin together. In a stable patient, the sequence may be exam, focused labs, then treatment. After the first interval update, reassess. CCS is dynamic. A patient who improves after bronchodilators still needs asthma education and trigger review. A patient with pneumonia who remains hypoxemic may need admission rather than discharge. A patient with abnormal uterine bleeding may need pregnancy testing before the case can safely move forward. Each update is a cue to refine management, not simply a reward screen. Track errors by category. Common categories include missed emergency orders, late treatment, unnecessary imaging, failure to monitor, wrong disposition, and missing preventive care. A raw case score is less useful than the pattern behind the score. If you repeatedly miss counseling, build a final two-minute checklist. If you repeatedly delay antibiotics, build a sepsis reflex. If you overorder CT scans in stable patients, practice outpatient diagnostic restraint. MDSteps can support this process by turning missed questions into automatic flashcard decks that are exportable to Anki. For CCS, the same principle applies: convert each missed management step into a short recall card. Example: “Young woman with lower abdominal pain in CCS: first safety test?” Answer: pregnancy test. These cards should be brief, order-focused, and linked to case triggers. Practice management decisions, CCS sequencing, live vitals, and weak-area review from one dashboard. Emergency orders are not memorized decorations. They are interventions that prevent deterioration while diagnostic information is pending. The most important CCS skill is recognizing when to act before complete certainty. The exam expects safe physician behavior, especially when delay would harm the patient. Use immediate stabilization for shock, severe respiratory distress, altered mental status, active seizure, suspected stroke within a treatment window, anaphylaxis, major trauma, myocardial infarction, diabetic ketoacidosis, severe hyperkalemia, meningitis, sepsis, and ectopic pregnancy concern. These presentations should trigger rapid monitoring and treatment. The exact orders depend on the syndrome, but the principle is constant: stabilize first, diagnose in parallel, reassess often. For respiratory distress, pulse oximetry and oxygen are common first steps when hypoxemia is present. Add bronchodilators for asthma or COPD exacerbation when the presentation supports bronchospasm. For pulmonary edema, consider nitrates and diuretics when appropriate, while monitoring hemodynamics. For suspected pulmonary embolism, risk stratification matters. A stable patient may need diagnostic imaging after pretest probability assessment, while an unstable patient requires urgent escalation. For circulatory instability, establish intravenous access and start fluids when volume depletion, sepsis, or hemorrhage is likely. Do not give large fluid volumes reflexively to every dyspneic patient. Heart failure and renal failure presentations require more caution. CCS favors tailored management over universal templates. One high-yield distinction is that CCS does not reward heroic therapy without indication. For example, oxygen is appropriate for hypoxemia or respiratory distress, not as an automatic order for every patient. Broad antibiotics are appropriate for suspected severe bacterial infection, not for uncomplicated viral syndromes. The best initial order strategy is decisive but still clinically disciplined. Time advancement is where CCS becomes different from ordinary question banks. Every order has a time cost, and the patient’s condition can change while tests are pending. Before advancing time, ask whether the patient is safe enough to wait. If not, treatment should start first or at the same time as diagnostic testing. For acute coronary syndrome, do not wait for troponin before obtaining an ECG or initiating appropriate antiplatelet therapy when the presentation is consistent and no contraindication is present. For meningitis, do not let imaging delay antibiotics when clinical urgency is high. For diabetic ketoacidosis, fluids and insulin strategy must be accompanied by electrolyte monitoring. For ectopic pregnancy concern, pregnancy testing and pelvic evaluation are essential, and unstable patients require urgent gynecologic management. For outpatient or chronic disease cases, time advancement is more forgiving, but closure is often where points are lost. A patient with newly diagnosed hypertension needs lifestyle counseling, follow-up, and screening for comorbid risk. A patient with diabetes needs glycemic assessment, kidney monitoring, eye and foot care, cardiovascular risk management, and immunization review. A patient with depression needs safety assessment, treatment planning, and follow-up. Do not confuse diagnostic breadth with diagnostic quality. A focused differential should drive test selection. In chest pain, myocardial infarction, pulmonary embolism, aortic dissection, pneumothorax, pneumonia, and reflux may all appear in the differential, but the presentation determines which tests come first. In abdominal pain, appendicitis, cholecystitis, pancreatitis, bowel obstruction, pregnancy-related emergencies, urinary stones, and vascular disease should be considered. CCS rewards recognizing the dangerous alternatives, not ordering every possible test. The final phase of a CCS case often separates adequate performance from excellent performance. Once the acute diagnosis is treated, the case may end early or enter a two-minute final order screen. This is the moment to add patient education, preventive care, risk-factor modification, medication reconciliation, follow-up, and monitoring. These steps must be clinically relevant. A patient admitted for septic shock does not need every outpatient screening order during the acute crisis, but a stable discharge case often does. Use final orders to address the condition that brought the patient in and the long-term risk that remains. For asthma, include inhaler technique, trigger avoidance, controller therapy when indicated, smoking cessation if relevant, and follow-up. For myocardial infarction, think secondary prevention, cardiac rehabilitation, lipid management, smoking cessation, and follow-up. For diabetes, think nutrition, exercise, glucose monitoring, kidney protection, eye care, foot care, and cardiovascular risk. For pregnancy-related cases, think prenatal care, medication safety, and warning signs. Preventive care should be age- and risk-appropriate. Adult immunizations, cancer screening, tobacco counseling, alcohol counseling, contraception counseling, fall prevention, and depression screening can matter in outpatient cases. However, CCS is not asking for a generic annual physical at the end of every case. The better habit is to ask: “What preventive action is directly relevant to this patient’s age, risks, diagnosis, and disposition?” A useful practice method is to create diagnosis-specific closure bundles. For example, “pneumonia discharge bundle” may include antibiotics, hydration advice, return precautions, smoking cessation, vaccine review, and follow-up. “DKA admission bundle” may include ICU or monitored setting, electrolyte monitoring, insulin protocol, fluids, glucose checks, potassium management, and diabetes education after stabilization. These bundles should be memorized as logic patterns, not rigid scripts. CCS preparation should begin early enough to build fluency but late enough that clinical knowledge is fresh. Four weeks is a practical structure for many residents and graduates who are also completing multiple-choice review. The goal is not to complete the maximum number of cases. The goal is to reduce preventable management errors. In the first week, learn the software and complete a small number of cases slowly. Focus on navigation, order entry, time advancement, and interpretation of interval updates. In the second week, increase case volume and build initial-order templates for emergencies, outpatient visits, and inpatient follow-up. In the third week, practice timed cases and track errors. In the fourth week, review weak syndromes, repeat missed cases, and rehearse final-order closure. Pair CCS work with multiple-choice review. Many Step 3 clinical decisions overlap with MCQ reasoning: stabilize first, diagnose dangerous conditions, treat promptly, avoid contraindications, and plan follow-up. The difference is that CCS forces the learner to execute every step. MDSteps can help by linking QBank misses, analytics, and readiness data into a study plan generator, so students can identify whether weak performance is coming from diagnosis, management, timing, or retention. During the last week, avoid making major strategy changes. Instead, standardize. Use the same first 30 seconds for every case. Use the same emergency screen. Use the same final-order checklist. The exam environment is not the place to invent a new workflow. It is the place to execute a practiced one. The final test-day mindset should be calm, structured, and safety-oriented. CCS cases can feel unpredictable because the patient evolves, but the physician task remains consistent. Identify acuity, stabilize when needed, test with purpose, treat without unsafe delay, reassess after interventions, and close the case with disposition and prevention. Remember the major CCS traps. Do not advance time in an unstable patient before starting therapy. Do not order invasive or risky tests without considering safer first steps. Do not forget pregnancy testing when it changes management. Do not treat chronic outpatient problems like emergencies. Do not discharge a patient who still needs monitoring, oxygen, intravenous therapy, or urgent consultation. Do not close a case without counseling when the diagnosis requires behavior change or medication adherence. CCS is best understood as a patient-safety exam. The best performers are not the students who type the longest order list. They are the students who know what must happen now, what can wait, and what must be completed before the patient leaves their care. With repeated timed practice, initial orders become less stressful because they come from a clinical framework rather than memory alone. Medically reviewed by: Daniel R. Castillo, MDWhy CCS Requires a Different Study Method
First priority
Second priority
Final priority
The Universal Initial Orders Framework
Presentation
Immediate orders
Focused diagnostics
Do not miss
Chest pain, unstable or concerning
IV access, cardiac monitor, oxygen if hypoxemic, aspirin if no contraindication
ECG, troponin, CBC, CMP, chest x-ray
Early ECG and reperfusion pathway when STEMI pattern appears
Fever, hypotension, suspected sepsis
IV access, fluids, blood pressure monitoring, broad antibiotics after cultures when feasible
CBC, CMP, lactate, blood cultures, urinalysis, chest x-ray as indicated
Do not delay antibiotics in unstable sepsis
Altered mental status
Airway assessment, glucose check, pulse oximetry, cardiac monitor
CMP, CBC, toxicology when indicated, CT head when focal signs or trauma
Check glucose early and treat reversible causes
Dyspnea
Pulse oximetry, oxygen if hypoxemic, cardiac monitor if severe
Chest x-ray, ECG, BNP or D-dimer when clinically appropriate
Distinguish asthma, heart failure, pneumonia, pulmonary embolism
Stable outpatient follow-up
Focused exam and medication reconciliation
Disease-specific labs and screening
Counseling, vaccines, follow-up, adherence barriers
How to Practice Cases Without Building Bad Habits
A practical three-pass review method
Turn this into Step 3 + CCS practice
Practice the sequence, not just the diagnosis.
Emergency Orders That Change Case Outcomes
Red-flag triggers
Stabilization logic
Diagnostics, Treatment, and Time Advancement
Situation
Advance now?
Reasoning
Unstable patient, no treatment started
No
Stabilization should precede waiting for tests.
Unstable patient, monitors and treatment started
Yes, short interval
Reassessment after intervention is appropriate.
Stable patient awaiting routine labs
Yes
Routine diagnostic processing is reasonable.
High-risk medication started
Only with monitoring
Check renal function, electrolytes, drug levels, or adverse effects when relevant.
Patient ready for discharge
After final orders
Complete counseling, prescriptions, follow-up, and return precautions first.
Final Orders, Prevention, and Case Closure
Final-order checklist
A Four-Week CCS Practice Plan
Week
Primary goal
Practice task
Review target
Week 1
Learn the interface
Complete cases untimed and write down order timing decisions
Navigation, order search, physical exam choices
Week 2
Build order frameworks
Practice emergency, outpatient, and inpatient cases
Initial stabilization and focused diagnostics
Week 3
Improve speed
Run timed cases and simulate real case transitions
Late treatment, overtesting, missed monitoring
Week 4
Polish closure
Repeat missed cases and rehearse final two-minute orders
Counseling, prevention, disposition, follow-up
Rapid-Review Checklist for Test Day
First 30 seconds
Final 2 minutes
References
CCS Cases
Best Step 3 CCS Practice and Initial Orders

Full access: $27/mo
Lifetime: $299
135 CCS casesStep 3 QBankManagement reasoning
Monthly access. Cancel anytime. 7-day good-faith refund after baseline + 100 QBank questions or 5 CCS cases.
CCS workflow
Still missing the same kinds of questions?
Read why that happens.
MDSteps exam-prep note: For Step 3 learners, live vitals CCS cases with timed orders and real physiology are especially useful because they train the exact sequence of recognizing instability, placing orders, advancing time, and reassessing response.