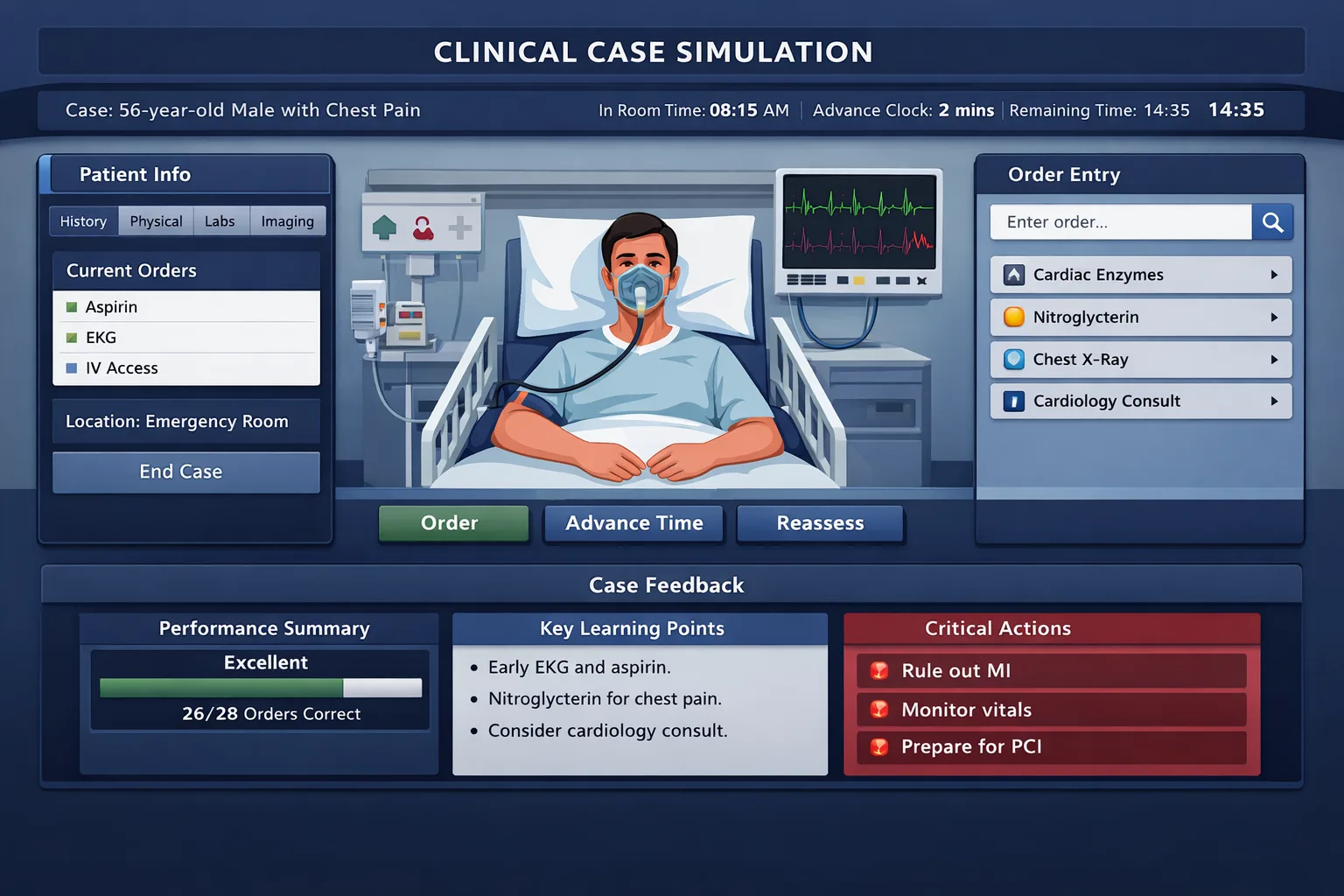
Affordable Step 3 CCS practice is not about finding the cheapest case list. It is about building a repeatable management system that helps a busy resident stabilize patients, choose the right setting, order efficiently, monitor response, and finish each simulation safely. Residents often think of Step 3 preparation as a resource problem. They compare subscriptions, question counts, case banks, and renewal fees. That comparison matters, especially when the exam fee, travel, scheduling changes, and lost post-call study time are already stressful. Yet the bigger cost in Computer-based Case Simulations is usually inefficient practice. A resident who completes many cases without a structured review system may spend weeks repeating the same errors: delayed stabilization, over-ordering, failing to change location, advancing time without reassessment, or ending without counseling and preventive care. CCS is different from multiple-choice studying because it tests management over time. The patient can improve, worsen, or reveal new information as simulated time advances. That design rewards clinicians who think in sequences. The right mental model is not “What is the diagnosis?” It is “Where should this patient be managed, what must be done now, what must be monitored, and what should happen before the case ends?” That is why low-cost preparation must focus on workflow. A smaller number of carefully reviewed cases can outperform a large, unfocused case binge. For residents on a budget, the first principle is to exhaust official orientation materials before paying for anything else. Official software exposure is not optional. The interface itself is part of the task. You need to know where orders go, how time advances, how interval history works, and how results are returned. A correct clinical plan can still lose value if it is entered late, entered in the wrong setting, or left unmonitored. The second principle is to separate clinical knowledge gaps from CCS mechanics gaps. If you miss acute coronary syndrome because you did not know the initial workup, that is a knowledge problem. If you knew the workup but forgot oxygen when hypoxemic, telemetry, aspirin when appropriate, serial ECGs, or admission to the correct level of care, that is a workflow problem. Each type of error needs a different fix. The most efficient budget strategy is therefore a layered plan: use free official materials for software familiarity, use a limited paid tool only when it provides timed realism and feedback, and maintain a personal error log organized by actions rather than diagnoses. The goal is not to memorize hundreds of scripts. The goal is to make safe, guideline-consistent actions automatic under time pressure. A resident’s CCS resource stack should be judged by whether it improves exam behavior. Case quantity alone is a weak metric. A case platform should help you practice free-text ordering, timed decision-making, simulated patient progression, reassessment, and end-of-case closure. If a resource only provides static reading, it may still be useful, but it should not be your only practice method. Start with official materials because they establish the exam interface and format. Then decide whether a paid simulator is necessary based on your baseline. If you are already comfortable with stabilization, order entry, time advancement, and counseling, you may need fewer paid cases. If you freeze when the case starts, forget setting changes, or advance time without checking vitals, a realistic simulator is worth prioritizing over another passive review book. The best affordable setup usually includes three components: official CCS orientation, a timed simulator, and an error tracking system. The error tracker can be a spreadsheet, notebook, or platform dashboard. Each entry should capture the missed action, the clinical trigger, and the corrected rule. For example: “Septic patient in ED, missed blood cultures before antibiotics when feasible, corrected rule: cultures, lactate, fluids, broad antibiotics, reassess perfusion.” This turns each miss into a reusable decision rule. MDSteps can fit this budget logic when residents want one integrated workspace rather than several disconnected tools. Its Step 3 live vitals CCS cases are designed around timed orders and real physiology, while the automatic study plan generator helps distribute limited study time across CCS, MCQs, and review. The value is strongest when you use the analytics to decide what to stop doing, not just what to do next. Every CCS case begins with a management problem, not a trivia question. The safest approach is to use a consistent opening sequence. First, identify acuity. Is the patient unstable, toxic, hypoxemic, hypotensive, altered, bleeding, septic, suicidal, or in severe pain? Second, choose the right location. An unstable patient belongs in the emergency department, inpatient unit, operating room, labor and delivery, or ICU depending on the scenario. Third, place immediate orders that protect the patient while diagnostic work proceeds. The early order set should be clinically appropriate, not automatic. In a crashing patient, consider airway, breathing, circulation, IV access, cardiac monitoring, pulse oximetry, oxygen if indicated, fluids or blood products when appropriate, ECG, bedside glucose, focused labs, imaging, cultures before antibiotics when feasible, analgesia, antiemetics, and specialty consultation when time-sensitive. In a stable outpatient, the first step may be focused history, physical examination, targeted tests, counseling, and follow-up rather than aggressive hospital orders. After initial management, the next habit is reassessment. CCS rewards physicians who monitor response. Do not advance time for hours after major interventions without checking interval history, vital signs, treatment response, and key results. If the patient improves, de-escalate logically. If the patient worsens, change location, broaden the differential, treat complications, or escalate care. The simulation is testing whether you can manage an evolving patient. Decide whether this is emergency, inpatient, ICU, outpatient, or home care. Protect airway, breathing, circulation, pain control, and immediate threats. Order targeted tests that match the leading differential and severity. Counsel, prevent recurrence, arrange follow-up, and discharge safely when appropriate. A practical case rhythm is: read the opening line, assign acuity, enter initial orders, perform focused examination, advance time only to the next meaningful result, reassess, treat definitively, reassess again, then close with counseling and follow-up. This prevents two common extremes. The first is diagnostic delay, where the resident orders tests but forgets to treat. The second is therapeutic overreach, where the resident orders broad treatments before confirming that the patient needs them. Practice management decisions, CCS sequencing, live vitals, and weak-area review from one dashboard. Paid CCS cases are most valuable when you treat them like exam rehearsals. Before starting a case, remove distractions, set a timer, and commit to finishing without pausing to look things up. During the case, act as you would on test day. After the case, slow down and review in detail. The learning happens after the simulation, when you identify which clinical cues you missed and which orders were delayed, unnecessary, or absent. A high-yield review should answer five questions. Did I choose the correct location? Did I stabilize before diagnosing? Did my diagnostic orders match the leading differential? Did I monitor response before advancing time? Did I close with prevention, counseling, and follow-up? These questions convert a broad performance score into fixable behaviors. Residents should avoid completing too many new cases in one sitting. Fatigue produces false data. A post-call resident who rushes through six simulations may conclude that the resource is not helping, when the real problem is poor attention. Two deeply reviewed cases can be more valuable than eight superficial ones. When time is limited, prioritize cases that represent common Step 3 settings: chest pain in the ED, dyspnea, abdominal pain, altered mental status, pregnancy-related concerns, pediatric fever, diabetes complications, trauma, depression or suicidality, and outpatient prevention. Use spaced repetition for CCS mechanics. Repeat a missed case after several days, but do not simply memorize the answer. Instead, rehearse the trigger-action rule. For example, “unstable upper GI bleed means two large-bore IVs, type and crossmatch, CBC, coagulation studies, fluids or blood as indicated, NPO, IV proton pump inhibitor when appropriate, GI consult, and monitoring.” The exact orders will vary, but the management logic becomes faster. For residents using MDSteps, missed CCS actions can be paired with the platform’s automatic flashcard decks from incorrect questions and cases. Exporting those misses to Anki can help convert repeated omissions into recall prompts. This is most useful for small, recurring failures such as forgetting pregnancy testing, smoking cessation counseling, vaccination review, medication reconciliation, or follow-up intervals. The first mistake is buying more resources before diagnosing the problem. If your CCS score feedback or practice review shows repeated omissions in stabilization, another case bank may not solve the issue. You need a front-loaded safety checklist. If your errors involve wrong diagnoses, then MCQ-style content review may be the better investment. If your errors involve timing, use software practice. Match the purchase to the deficit. The second mistake is treating CCS like an oral board script. CCS is interactive. You are not rewarded for writing a beautiful assessment. You are rewarded for patient-centered actions entered into the case system. A resident may know that a patient has diabetic ketoacidosis, but the simulation needs orders: fluids, insulin when potassium is safe, electrolyte monitoring, glucose monitoring, precipitant evaluation, and appropriate disposition. Knowledge must become action. The third mistake is over-ordering because “more feels safer.” In real practice and on the exam, unnecessary invasive tests, irrelevant imaging, and inappropriate treatments can signal poor judgment. A broad initial workup is appropriate in unstable or undifferentiated patients, but indiscriminate ordering is not. Ask whether each order changes diagnosis, treatment, monitoring, disposition, or prevention. If it does not, reconsider it. The fourth mistake is forgetting outpatient logic. Not every CCS case is an emergency. Some cases test prevention, chronic disease management, medication adjustment, risk-factor counseling, screening, adherence, and follow-up. An outpatient with uncontrolled hypertension does not automatically need admission. A stable patient with depression needs safety assessment, treatment planning, counseling, and follow-up. A child with routine findings may need reassurance, parental education, immunization review, or return precautions. The fifth mistake is ignoring closure. End-of-case actions often reflect real physician behavior: counsel the patient, stop harmful medications, arrange follow-up, address preventive care, document lifestyle counseling, and give return precautions. These actions are easy to forget because they occur after the diagnostic “answer” is obvious. Build a final 60-second closure ritual into every case. A resident schedule must respect clinical reality. Long daily study blocks are often unrealistic during wards, nights, ICU rotations, or outpatient continuity weeks. The better plan is to combine short weekday drills with longer weekend review. CCS preparation does not require perfection every day. It requires repeated exposure to the same management sequence until it becomes automatic. Week 1 should focus on software and system building. Complete the official orientation materials and practice cases. Create your initial order framework for unstable patients, stable outpatient presentations, pediatric cases, obstetric cases, psychiatric safety cases, and chronic disease follow-up. Do not over-polish these templates. They are scaffolds, not scripts. Week 2 should focus on timed practice. Complete several cases under exam-like conditions. After each case, write down missed actions using a three-column log: trigger, missed action, corrected rule. Avoid vague notes such as “review cardiology.” Write “chest pain with diaphoresis, missed serial troponin and repeat ECG, corrected rule: monitor evolving ACS even after initial testing.” Week 3 should focus on weak settings. If you struggle with ICU escalation, practice unstable cases. If you struggle with ambulatory prevention, practice outpatient cases. If you struggle with pregnancy, pediatrics, psychiatry, or infectious disease, target those areas. Add brief MCQ review for the underlying clinical topics so your CCS actions rest on solid knowledge. Week 4 should focus on speed, closure, and confidence. Repeat missed cases, rehearse your final counseling checklist, and reduce new resource intake. The week before the exam is not the time to buy another large resource. It is the time to sharpen execution. On exam day, CCS performance depends on calm repetition. You should not be inventing your system during the test. Use a simple, durable checklist that fits nearly every case. The checklist should not replace clinical judgment. It should prevent avoidable omissions when fatigue rises late on Day 2. NBME-style traps often involve timing and safety rather than rare diagnoses. A patient with chest pain may need immediate stabilization and ACS evaluation before an exotic differential. A febrile child may require age-appropriate sepsis thinking. A pregnant patient with abdominal pain requires fetal and maternal considerations. A psychiatric patient requires safety assessment before routine discharge. A patient who improves after treatment still needs appropriate follow-up and prevention. The strongest residents treat the case like a real shift. They do not wait for perfect certainty before treating emergencies, and they do not hospitalize stable patients without reason. They reassess after interventions. They avoid harmful orders. They remember that the case can end early when management is appropriate. That early ending should be interpreted calmly, not as a reason to panic. A lean Step 3 CCS plan can be highly effective if it is disciplined. Start free, pay only for the features that change your behavior, and review every miss until it becomes a rule. Residents do not need a luxury stack of resources to pass CCS. They need interface familiarity, safe management habits, enough timed practice to reduce hesitation, and an honest record of repeated mistakes. When deciding whether a paid CCS tool is worth it, ask four questions. Does it simulate the time pressure of the exam? Does it require free-text or exam-like ordering? Does it provide feedback specific enough to change my next case? Does it help me track patterns across cases? If the answer is yes, the tool may be worth the cost. If the answer is no, another free or low-cost method may be better. Budget preparation also means protecting your attention. Do not study CCS only when exhausted. Put short drills into predictable windows: one case after clinic, one review block on a lighter day, one weekend session for repeated misses. Use commute or downtime for order-set recall, but reserve actual cases for focused practice. CCS is procedural memory. It improves when practice conditions resemble test conditions. Finally, remember what Step 3 is measuring. The exam is designed for physicians moving toward unsupervised practice. CCS evaluates whether you can manage a patient over time, respond to changing information, and make safe decisions in varied settings. That is the same skill residents use on call, in clinic, and during handoffs. Studying well for CCS should make you more systematic clinically, not just more prepared for a software simulation. If you use MDSteps, keep the workflow practical: build a study plan, complete live vitals CCS cases, review analytics, convert misses into flashcards, and return to weak areas before buying anything else. The best resource is the one that makes your next case safer, faster, and more organized. Medically reviewed by: Elena Ramirez, MD, FACPWhy CCS Feels Expensive When Time Is the Real Cost
A Budget Framework for Choosing CCS Resources
Resource Type
Best Use
Budget Value
Common Pitfall
Official CCS practice software
Interface familiarity, order entry, timing mechanics
Highest starting value
Using it once passively instead of rehearsing workflow
Timed CCS simulator
Building speed, monitoring habits, closure routines
High if feedback is specific
Chasing case volume without reviewing misses
Question bank
Filling diagnosis and management gaps
Moderate to high
Assuming MCQ improvement automatically fixes CCS behavior
Self-made order templates
Turning repeated actions into automatic checklists
Very high
Using rigid templates when the patient needs individualized care
The Core CCS Algorithm Residents Should Rehearse
Acuity
Stabilize
Diagnose
Close
Turn this into Step 3 + CCS practice
Practice the sequence, not just the diagnosis.
How to Practice Without Wasting Paid Cases
Common Budget Mistakes That Lower CCS Performance
A Four-Week Low-Cost CCS Study Schedule
Week
Primary Goal
Resident-Friendly Task
Success Marker
1
Learn interface
Official CCS tutorial plus 2 practice cases
You can enter orders and advance time without hesitation
2
Build timing
4 to 6 timed cases with review
You reassess after major interventions
3
Target weaknesses
Focused cases by setting and diagnosis group
Your error log shows fewer repeated omissions
4
Polish closure
Repeat missed cases and final-order drills
You consistently counsel, prevent, and arrange follow-up
Rapid-Review Checklist for CCS Case Day
CCS Rapid-Review Checklist
How to Spend Less and Still Prepare Seriously
References
CCS Cases
Step 3 On a Budget: Affordable CCS Strategies that work.

Full access: $27/mo
Lifetime: $299
135 CCS casesStep 3 QBankManagement reasoning
Monthly access. Cancel anytime. 7-day good-faith refund after baseline + 100 QBank questions or 5 CCS cases.
CCS workflow
Still missing the same kinds of questions?
Read why that happens.