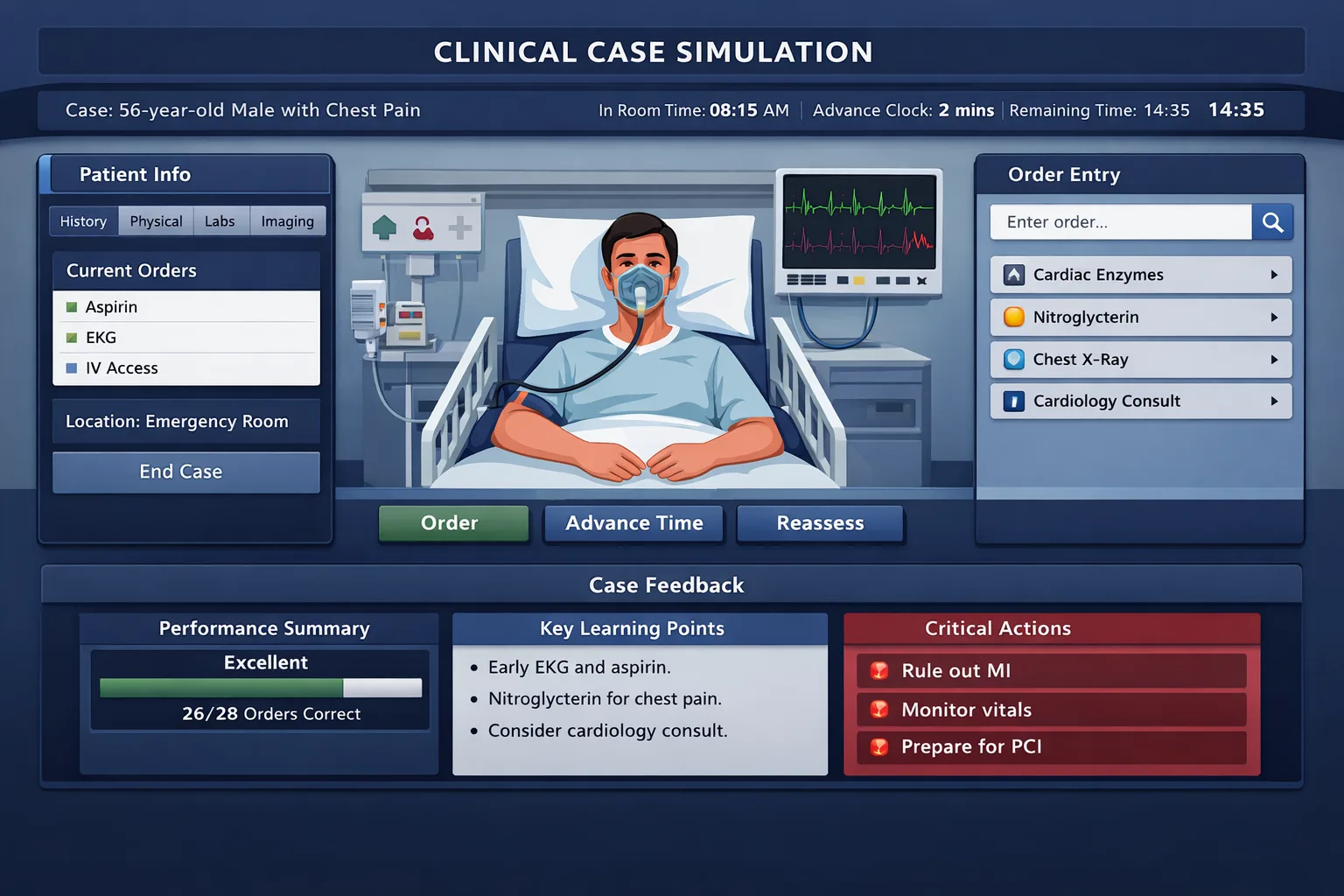
Learn why a Step 3 CCS case may stop before the clock runs out, how to interpret that ending, and how to avoid over-ordering when the patient has already improved. CCS cases ending early on the real test usually feels more dramatic than it is. CCS cases ending early on the real test usually feels more dramatic than it is. A case that closes with time left does not automatically mean failure, a missed diagnosis, or a software problem. The official Step 3 CCS format is built around simulated patient management, not around forcing every examinee to use the full clock. Some cases are allotted a maximum of 10 or 20 minutes of real time, but a case may require less time if the key clinical management decisions have already been made. The safer interpretation is this: the case has reached an endpoint in the simulation. That endpoint may occur after the patient stabilizes, after the needed diagnostic and therapeutic sequence is complete, or after the system has enough information about your management pattern. The exam is not asking whether you can keep ordering until the clock expires. It is asking whether you can identify the clinical task, sequence care safely, and stop adding actions that do not change management. This matters because students often react to an early ending with the wrong post-test story. They assume, “It ended fast, so I must have killed the patient,” or “It ended fast, so I must have done perfectly.” Neither conclusion is reliable. A short case may reflect efficient management, but it can also reflect a case where the patient deteriorated after delayed or harmful care. The only useful question is whether your orders matched the patient’s changing physiology. Core rule: Early closure is a timing signal, not a score report. Judge your performance by stabilization, diagnostic confirmation, treatment, monitoring, and disposition. The key distinction is whether the patient was moving in the right clinical direction before the case ended. The key distinction is whether the patient was moving in the right clinical direction before the case ended. A reassuring early finish usually follows a coherent chain: you recognized the site of care, addressed unstable vital signs, ordered focused diagnostic tests, gave definitive treatment, reassessed the patient, and set the correct disposition. For example, an emergency department patient with hypoxia and pneumonia should receive oxygen when indicated, appropriate studies, antibiotics, reassessment, and admission if clinically necessary. If the patient improves and the case closes, that early stop is less concerning. A dangerous early ending has a different pattern. The case may close after a critical omission, such as failing to treat shock, missing airway compromise, discharging an unstable patient, or delaying therapy while waiting for confirmatory tests. In CCS, the patient’s condition can change as simulated time passes. That means the wrong clock move can be just as harmful as the wrong medication. Advancing time before reassessment in an unstable patient is a common Distractor Trap because it feels efficient, but it hides clinical deterioration. Use the following table after practice cases and after your real exam recall. It prevents emotional interpretation and forces a management audit. This is the same reasoning layer used in MDSteps CCS practice, where live vitals and timed orders help students see whether their sequence is clinically safe, not just whether their diagnosis is correct. An early case ending is easier to interpret when you review it through the MDSteps Reasoning Method. An early case ending is easier to interpret when you review it through the MDSteps Reasoning Method. Start with the exam task. Is this an urgent intervention case, an initial workup case, or a continuing-care case? A patient with chest pain, hypotension, fever, altered mental status, severe dyspnea, neurologic deficit, pregnancy complication, trauma, or pediatric instability is not primarily a “diagnosis case.” It is a safety and sequencing case. Next, find the Pivot Clue. In CCS, the Pivot Clue is often not a rare finding. It is the vital sign, location, time course, or response to treatment that changes what must happen next. Oxygen saturation of 82%, systolic blood pressure below 90 mm Hg, fever with neck stiffness, postpartum hemorrhage, or new unilateral weakness should move you from leisurely testing to immediate stabilization. The Distractor Trap is usually a familiar order that is true but not first. A CT, culture, consult, or outpatient follow-up may be appropriate eventually, but unsafe if it delays immediate care. Treat airway, breathing, circulation, pain, glucose, fever, pregnancy risk, or sepsis physiology before large time jumps. Order focused tests that prove the working diagnosis and identify complications that change management. Reassess, monitor, counsel, add prevention when appropriate, and choose disposition based on risk. Finally, classify the miss pattern. Did you know the diagnosis but delay treatment? Did you order treatment but forget monitoring? Did you admit correctly but skip preventive care? Each miss should become one Takeaway Rule, such as “Do not advance hours in an unstable patient without reassessing vitals and treatment response.” The final minutes of a CCS case create a specific kind of anxiety. The final minutes of a CCS case create a specific kind of anxiety. Students start adding orders because silence feels unsafe. This is where many points are lost. Over-ordering can signal poor judgment when tests are invasive, irrelevant, expensive, delayed, or risky. The goal is not to empty a memorized order set. The goal is to demonstrate that you know what the patient needs next. When the patient is improving, shift from rescue mode to closure mode. Recheck interval history and focused physical findings if they will change care. Review key results. Continue indicated therapy. Add monitoring only when it matches the diagnosis. Then choose the correct site of care. A stable outpatient with mild disease may need discharge instructions and follow-up. A patient with persistent hypoxia, sepsis physiology, myocardial ischemia, stroke symptoms, suicidal intent, or surgical abdomen should not be sent home because the first treatment helped. Do not confuse “case has not ended yet” with “I must be missing ten orders.” Sometimes the system is giving you time to complete disposition, counseling, screening, or follow-up. Other times, it is testing whether you will create harm by ordering unnecessary procedures. For Step 3, the generalist role matters. You can consult when appropriate, but you should not use consultation as a substitute for initial management. MDSteps CCS cases are designed to make this visible through timed orders, live vitals, and real physiology, so students can practice stopping safely instead of practicing longer order lists. On test day, your mental script should be simple. On test day, your mental script should be simple. When a case ends early, do not carry the emotional reaction into the next case. You will not receive a real-time score explanation, and the ending itself is not enough information to grade yourself. The best response is to reset and apply the same management framework to the next patient. Before the exam, train with a post-case audit rather than a post-case mood. Write down the clinical task, the Pivot Clue, the first treatment decision, the monitoring step, and the disposition. If you repeatedly find that you knew the diagnosis but forgot reassessment, your Reasoning Profile is not “weak topic knowledge.” It is a sequencing problem. If you repeatedly order large panels before treating unstable physiology, your pattern is stabilization delay. If you repeatedly finish with the right treatment but no follow-up or counseling, your pattern is incomplete closure. Unstable firstFocused testsTreat earlyMonitor responseClose safely A strong CCS performance is not defined by the number of orders. It is defined by whether each order matches the patient’s risk at that moment. The practical goal is to leave each case knowing that your actions formed a safe sequence. If a short case followed stabilization, focused confirmation, definitive therapy, reassessment, and appropriate disposition, do not punish yourself for not using the whole clock. If it ended after a skipped safety step, turn that into a practice target. The exam rewards clinical management under time pressure, not perfectionism after the patient is already managed.Why a CCS Case Can Stop Before Time Runs Out
Separate a Good Early Ending From a Dangerous One
Student symptom
Likely reasoning problem
MDSteps-style fix
Case ended early and patient had not been reassessed
Clock advancement replaced monitoring
Make reassessment a Takeaway Rule before large time jumps
Case closed after many broad orders
Over-ordering masked the core task
Identify the Pivot Clue before adding low-yield tests
Case ended after treatment but no disposition
Management stopped before final safety step
Convert the diagnosis into admission, discharge, follow-up, or transfer
The MDSteps Reasoning Method for Early CCS Endings
1. Stabilize
2. Confirm
3. Close safely
What Not to Do When the Case Feels Almost Finished
Safe closure screen
Exam-Day Essentials for Early CCS Endings
Rapid-review checklist
Takeaway Rules
References
CCS is not just what you order. It is when you order, reassess, and close the case.
MDSteps helps you practice live CCS cases with vitals, orders, labs, time advancement, reassessment, closure, and after-action feedback.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.