Understand What CCS Rewards Before You Practice
Step 3 CCS scoring is best approached as a patient-management exercise, not as a hidden checklist of obscure orders.
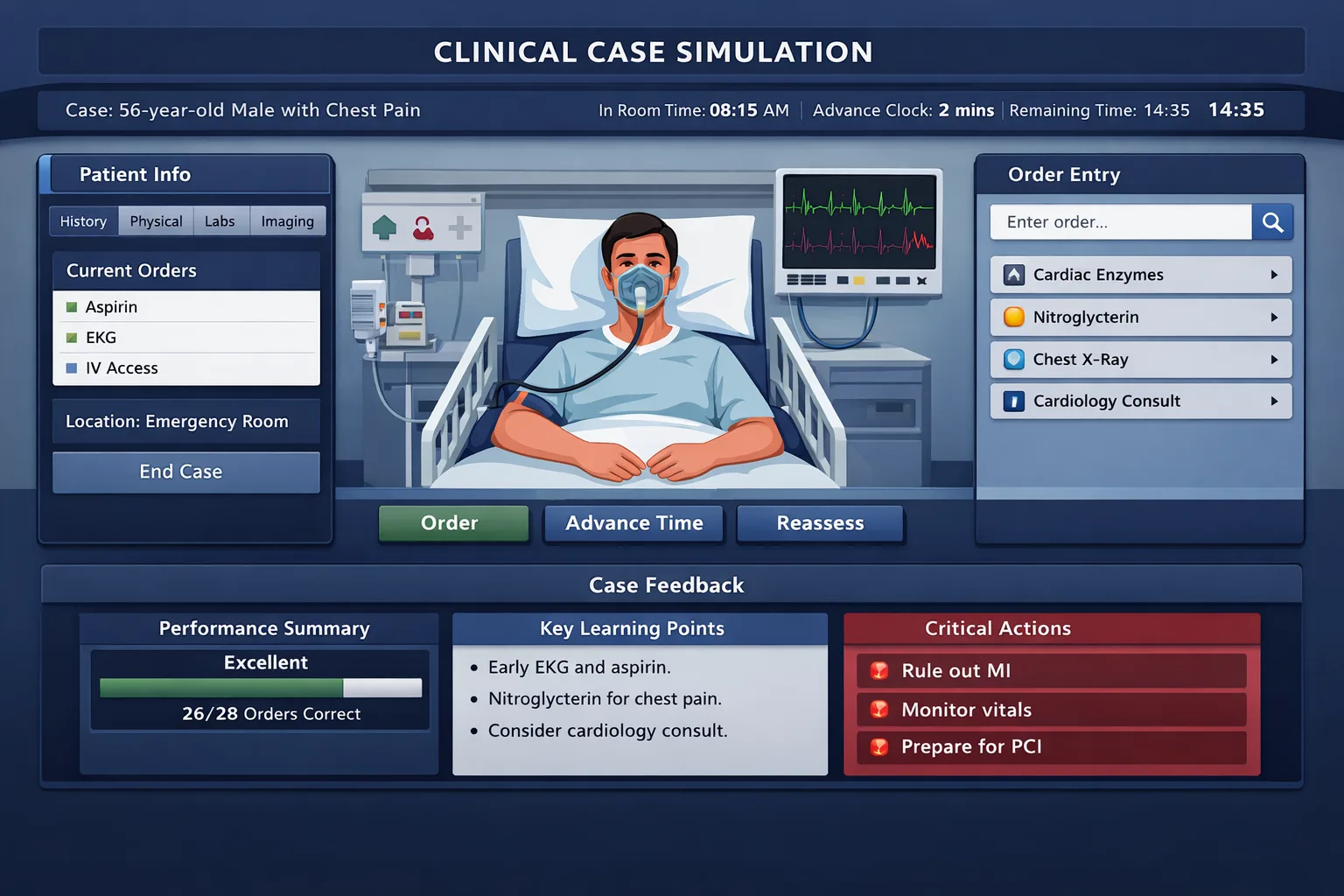
Step 3 CCS scoring is best approached as a patient-management exercise, not as a hidden checklist of obscure orders. The official USMLE materials describe Computer-based Case Simulations as encounters in which the examinee manages a patient over simulated time using the Primum software. That design matters. A strong performance comes from making safe, timely, clinically justified decisions while the patient evolves. The case is asking whether you can act like an independently responsible physician who can stabilize, investigate, treat, monitor, and dispose of a patient in an appropriate care setting.
The first mistake students make is treating CCS like a multiple-choice question with extra typing. A multiple-choice item usually rewards choosing the best next step after reading a vignette. A CCS case rewards a sequence. You must decide what information is urgent, what orders are time sensitive, what therapies should begin before confirmatory testing, when to advance the clock, when to reassess, and when the patient should be admitted, transferred, discharged, or counseled. The case is dynamic. If you order an intervention but never reassess, you have not shown the system that you are monitoring response. If you diagnose the condition but fail to move the patient to the proper location, the management plan remains incomplete.
The useful mental model is simple: the software evaluates whether your actions are medically appropriate for the patient’s evolving condition. Your goal is not to order everything. Your goal is to order the right things early, avoid dangerous or unnecessary actions, and demonstrate closure. Closure means you handled the acute problem, prevented foreseeable harm, arranged definitive management, and addressed relevant prevention before the case ends.
High-yield rule: In CCS, correct diagnosis is not enough. Performance improves when diagnosis is paired with early stabilization, targeted testing, active treatment, reassessment, and appropriate final disposition.
For example, a patient with chest pain and diaphoresis is not just a “myocardial infarction case.” It is a timing case. The early actions should reflect ABCs, vital sign review, cardiac monitoring, oxygen only when indicated, aspirin when appropriate, ECG, troponin testing, IV access, pain control, anticoagulation when indicated, and rapid reperfusion planning if ST-elevation is present. A learner who waits for every laboratory result before acting can lose credit for delayed care. A learner who orders broad testing without ECG, monitoring, or treatment misses the core clinical priority.
The same logic applies to sepsis, DKA, ectopic pregnancy, asthma exacerbation, meningitis, acute stroke, upper gastrointestinal bleeding, and hypertensive emergency. The CCS interface can make these problems feel artificial, but the scoring logic follows bedside priorities. A severely ill patient should not remain in an outpatient office. A patient requiring continuous monitoring belongs in the emergency department, inpatient unit, ICU, operating room, labor and delivery, or another suitable setting. A stable patient who needs outpatient workup should not be admitted reflexively. Matching acuity to location is one of the simplest ways to improve case performance.
Students also overestimate the value of rare diagnoses and underestimate routine care. CCS cases commonly test common, dangerous, and time-sensitive scenarios. The exam favors broad independent practice. You should know what to do when the patient presents with shortness of breath, fever, abdominal pain, altered mental status, trauma, pregnancy-related symptoms, chest pain, syncope, renal failure, intoxication, or postoperative complications. Your case pattern should begin with safety, not with a long differential list. Differential diagnosis matters because it guides testing, but early actions should be anchored to what can harm the patient in the next few minutes or hours.
The practical implication is that your preparation should include two tracks. First, build illness scripts for common CCS presentations. Second, practice the mechanics of the software until order entry, clock advancement, reassessment, and location changes become automatic. A candidate who knows medicine but fights the interface wastes time and misses follow-up actions. A candidate who understands the interface but lacks management logic places scattered orders. The winning combination is clinical judgment plus procedural fluency.
Build a Case Framework Around Stabilize, Diagnose, Treat, Reassess
A reliable CCS framework reduces cognitive load.
A reliable CCS framework reduces cognitive load. Under test pressure, students often forget obvious orders because they are thinking about the final diagnosis too early. The better habit is to run every case through a consistent sequence: stabilize, diagnose, treat, reassess, and close. This sequence does not mean every patient receives the same orders. It means every patient is managed through the same clinical logic.
Stabilization begins with the patient’s location and acuity. A patient in respiratory distress, shock, severe pain, altered mental status, acute neurologic deficit, active bleeding, or unstable arrhythmia should usually move to a higher-acuity setting. Emergency care is not only about ordering tests. It is about placing the patient where frequent vitals, monitoring, nursing response, and urgent procedures can occur. Students lose performance by leaving unstable patients in clinic or by sending them home after partial improvement.
Diagnostic work should be targeted. CCS does not reward thoughtless “pan-ordering.” Broad panels may be appropriate for shock, sepsis, toxic ingestion, or severe undifferentiated illness, but not for every outpatient complaint. A young stable patient with classic cystitis does not need a CT abdomen, blood cultures, and admission. A patient with suspected pulmonary embolism may need pregnancy testing, oxygen saturation assessment, ECG, chest radiograph, D-dimer or CT pulmonary angiography depending on probability, anticoagulation if clinical risk is high, and monitoring. The workup should fit the pretest probability and danger of the condition.
Stabilize
ABCs, vitals, IV access, monitoring, oxygen when indicated, fluids or urgent therapy.
Diagnose
Order focused labs, imaging, cultures, ECG, pregnancy test, or procedure based on risk.
Treat
Start time-sensitive therapy before late confirmation when delay is unsafe.
Reassess
Advance time, review results, repeat vitals, adjust therapy, and arrange disposition.
Treatment sequencing is a major score differentiator. In meningitis, blood cultures should not create a harmful delay in antibiotics. In DKA, fluids and insulin matter, but potassium status must be checked and corrected appropriately. In asthma exacerbation, bronchodilators and systemic corticosteroids should be started early, with escalation if response is poor. In suspected ovarian torsion, definitive gynecologic intervention matters more than a prolonged outpatient workup. CCS cases often reveal whether the examinee understands when treatment is urgent and when observation is reasonable.
Reassessment is where many competent students lose points. After ordering fluids, repeat vital signs. After bronchodilators, check respiratory status and oxygen saturation. After antihypertensive therapy, reassess blood pressure and symptoms. After transfusion, monitor hemoglobin, vitals, and clinical response. After antibiotics, follow temperature, hemodynamics, and culture results. The software cannot infer that you are monitoring unless you order or request follow-up actions and advance simulated time appropriately.
Closure means the case has a safe endpoint. Some cases end automatically after correct management, but you should still build the habit of finishing with disposition and prevention. Admit when needed. Transfer to ICU, operating room, or labor and delivery when the patient requires it. Discharge only after stability, diagnosis, treatment, instructions, follow-up, and return precautions. Add counseling that fits the case: smoking cessation, medication adherence, diabetic education, safe sex counseling, injury prevention, diet, exercise, alcohol reduction, or vaccination when relevant. These actions are not decorative. They demonstrate comprehensive care.
The key is flexibility. The framework is stable, but each case changes the details. A stable outpatient with hypertension needs confirmation, risk assessment, lifestyle counseling, medication initiation when indicated, and follow-up. A patient with hypertensive emergency needs acute end-organ evaluation, controlled blood pressure reduction, monitoring, and admission. The diagnosis may look similar, but the management pathway differs because acuity differs. That distinction is central to CCS case performance.
Orders That Usually Move the Needle
High-performing CCS examinees do not memorize one universal order set.
High-performing CCS examinees do not memorize one universal order set. They memorize clinical categories. The correct order depends on the patient, but the categories recur: safety, monitoring, access, diagnostic confirmation, therapeutic intervention, consultation, prevention, and follow-up. This approach prevents both under-ordering and indiscriminate over-ordering.
Safety orders are the first category. They include vital signs, pulse oximetry, cardiac monitoring, IV access, bed rest when appropriate, fall precautions, isolation precautions, NPO status before procedures, and pregnancy testing when reproductive-age patients might receive imaging or teratogenic treatment. Safety also includes avoiding harmful orders. Do not give beta blockers in unstable cocaine-associated chest pain without careful context. Do not give thrombolysis without checking contraindications. Do not delay antibiotics for unstable sepsis. Do not send a patient with active suicidal ideation home without safety evaluation.
Monitoring orders show that you are following the patient’s course. They are especially important in acute cases. Repeat vital signs, intake and output, glucose checks, neurologic checks, cardiac rhythm monitoring, urine output, oxygen saturation, and repeat targeted labs can be decisive. A case of DKA is not managed by one glucose level and one insulin order. It requires fluids, electrolyte monitoring, insulin titration, potassium management, anion gap follow-up, and transition planning. A case of GI bleeding requires hemodynamic monitoring, type and screen or crossmatch, serial hemoglobin, resuscitation, endoscopic evaluation when indicated, and disposition.
| Clinical scenario | Early actions | Common missed performance actions |
|---|---|---|
| Unstable chest pain | ECG, monitoring, IV access, aspirin when appropriate, troponin, reperfusion pathway if STEMI | Forgetting repeat ECG, cardiology consult, admission level, risk-factor counseling |
| Sepsis or shock | High-acuity setting, cultures when feasible, broad antibiotics, fluids, lactate, source evaluation | Waiting too long for tests, no urine output monitoring, no ICU escalation |
| DKA | Fluids, electrolytes, glucose, ketones, venous blood gas, insulin when potassium is safe | No potassium reassessment, no anion gap follow-up, premature discharge |
| Acute asthma | Oxygen if hypoxemic, bronchodilators, systemic steroids, reassessment, escalation if severe | No repeat respiratory exam, no peak flow, no admission decision after poor response |
| Pregnancy pain or bleeding | Pregnancy test, ultrasound when indicated, hemodynamic assessment, OB/GYN involvement | Missing Rh status, failing to recognize ectopic risk, delayed procedure or transfer |
Therapeutic orders must match severity. In outpatient cellulitis, oral antibiotics and follow-up may be enough. In necrotizing infection, broad antibiotics, urgent surgery, fluids, cultures, and ICU-level care may be required. In simple migraine, symptomatic treatment and discharge instructions may be appropriate. In sudden thunderclap headache, the workup must address subarachnoid hemorrhage. The board-style trap is that similar symptoms can require very different management if red flags are present.
Consultations should not replace management. Calling surgery for appendicitis is appropriate, but the patient still needs NPO status, IV fluids, pain control, antibiotics when indicated, labs, imaging strategy, and disposition. Calling cardiology for STEMI is appropriate, but aspirin, anticoagulation strategy, monitoring, and reperfusion logistics still matter. A consultant is a bridge to definitive care, not a substitute for initial physician action.
Preventive and counseling orders are often remembered at the end, but they should not be random. Counseling should fit the diagnosis. A COPD exacerbation case may need smoking cessation, inhaler technique, vaccines, pulmonary follow-up, and avoidance of triggers. A sexually transmitted infection case may need partner treatment, safe sex counseling, HIV testing, and pregnancy considerations. A diabetic case may need foot care, eye care, renal screening, glucose monitoring education, diet, and follow-up. These details help close the loop after acute management.
To improve CCS case performance, practice writing orders in categories rather than lists. After each case, ask: Did I protect the patient? Did I obtain the decisive information? Did I treat the dangerous process early enough? Did I monitor response? Did I move the patient to the right location? Did I arrange follow-up and prevention? If one category is repeatedly weak, that category becomes the next practice target.
Timing, Clock Management, and Reassessment
The CCS clock is not a passive timer. It is a clinical tool.
The CCS clock is not a passive timer. It is a clinical tool. Advancing time too early can harm performance because the patient may deteriorate before essential therapy begins. Refusing to advance time can also harm performance because the case cannot show improvement, new results, or the need for escalation. The skill is knowing when the patient is safe enough for time to pass.
Before advancing the clock in an acute case, confirm that immediate danger has been addressed. For a hypotensive patient, that may include IV access, fluids, monitoring, oxygen if indicated, urgent labs, and appropriate empiric therapy. For a patient with suspected stroke, it may include glucose check, neurologic assessment, CT head, time of onset, blood pressure assessment, and stroke team involvement. For an unstable arrhythmia, it may include cardiac monitoring, ACLS-based intervention, electrolytes, and appropriate disposition. Once essential actions are placed, advancing time allows results and clinical response to appear.
The second timing skill is reassessment after intervention. Students often place correct orders but never check whether those orders worked. The patient with asthma receives nebulized treatment, but the examinee does not repeat lung exam or oxygen saturation. The patient with sepsis receives fluids, but no repeat blood pressure, urine output, lactate trend, or vasopressor escalation occurs. The patient with hyperkalemia receives calcium, insulin, glucose, and albuterol, but no repeat potassium or ECG follow-up is ordered. These are not minor omissions. They are evidence that the physician has not completed the management cycle.
Clock management also affects diagnostic sequencing. Some tests return quickly, such as ECG, bedside glucose, urinalysis, pregnancy test, chest radiograph, or basic labs. Others take longer or require procedural scheduling. If a patient needs immediate therapy, do not wait for slow tests before treating. If a patient is stable and the diagnosis depends on imaging or laboratory confirmation, advancing to results is appropriate after safety measures are in place. Think like a clinician: what can safely wait, and what cannot?
There is also a disposal timing problem. Some students discharge too early because symptoms improve. Improvement is not always safety. A patient with transient ischemic attack still needs risk evaluation and prevention. A patient with syncope may need cardiac workup if red flags exist. A patient with ectopic pregnancy cannot be reassured after transient pain improvement. A patient with severe depression and suicidal ideation needs safety planning and psychiatric evaluation. CCS rewards appropriate disposition, not quick endings.
Advance time when
Immediate stabilization is complete, initial treatment is active, and you are waiting for response or results.
Pause time when
The patient is unstable, a critical order is missing, or deterioration would be foreseeable.
Reassess after
Fluids, oxygen, bronchodilators, insulin, antibiotics, antihypertensives, transfusion, procedures, or transfer.
A useful drill is to pause after every simulated time jump and ask three questions. What changed? What result returned? What new action is now required? If vital signs improved, you may narrow treatment, continue monitoring, or plan disposition. If vitals worsened, you must escalate. If a test confirms the diagnosis, order definitive treatment. If a test rules out your leading diagnosis, return to the differential. This prevents the common error of continuing a prewritten plan even after the case has changed.
Timed orders are one reason simulation practice is more valuable than passive reading for CCS. Reading that sepsis needs antibiotics is easy. Managing a simulated patient who becomes hypotensive after an inadequate fluid response forces you to practice escalation. This is where MDSteps live vitals CCS cases can be useful for Step 3 candidates because timed orders interact with changing physiology. The point is not to memorize a single pathway. The point is to train the timing decisions that static answer explanations cannot fully reproduce.
Strong timing performance looks calm. You place urgent orders early, advance to meaningful intervals, reassess response, and adjust. Weak timing performance looks either frantic or frozen. Frantic candidates order everything and jump around. Frozen candidates overthink diagnosis and avoid advancing time. The best examinees act, observe, and refine.
Avoid the Errors That Quietly Lower Performance
Many CCS losses are not caused by rare knowledge gaps.
Many CCS losses are not caused by rare knowledge gaps. They come from repeated small errors that show unsafe or incomplete care. The most common pattern is delayed stabilization. A patient is unstable, but the examinee starts with a long diagnostic workup. In real practice, diagnosis and stabilization often happen together. In CCS, that parallel process should be visible in the orders. Vitals, monitoring, IV access, oxygen when indicated, fluids, glucose check, ECG, or emergent therapy may need to occur before the full differential is settled.
The second pattern is wrong setting. Location matters because it reflects acuity. A patient with active chest pain and abnormal ECG does not belong in an office. A patient with respiratory failure does not belong in routine outpatient follow-up. A patient requiring surgery needs operative or specialty pathways. A stable patient with mild disease may be safely managed as an outpatient. Moving every patient to the hospital is not a strategy. Matching the setting to risk is the strategy.
The third error is “diagnosis without management.” A student identifies pneumonia but forgets oxygen assessment, severity evaluation, antibiotics, blood cultures when indicated, admission criteria, or follow-up. Another identifies acute coronary syndrome but forgets antiplatelet therapy, anticoagulation strategy, monitoring, cardiology involvement, and risk-factor treatment. CCS is not asking whether you can name the disease. It is asking whether you can run the case.
The fourth error is over-ordering. Excessive testing can signal poor judgment, especially in stable outpatient cases. Ordering invasive tests, broad imaging, or unnecessary antibiotics can be harmful. Avoid “kitchen sink” behavior. A patient with uncomplicated viral upper respiratory symptoms does not need CT imaging, blood cultures, and broad-spectrum antibiotics. A patient with benign musculoskeletal pain does not need a massive inpatient workup unless red flags exist. The exam favors appropriate care, not maximum care.
The fifth error is neglecting contraindications. Before anticoagulation, thrombolysis, procedures, teratogenic medications, or imaging with radiation, consider pregnancy status, bleeding risk, renal function, allergy, medication interactions, and procedural contraindications. This is where Step 3 differs from earlier exams. It assumes you can manage risk, not just identify mechanisms.
The sixth error is failing to address patient comfort. Pain control, antiemetics, antipyretics, bronchodilators, fluids, anxiolysis when appropriate, and supportive care are part of management. Do not let the patient suffer while you chase diagnostic certainty. Comfort orders should be clinically safe and appropriate. They also show that you are treating the patient, not only the disease.
NBME-style trap: If a patient improves after initial treatment, the case may still require definitive care. Improvement does not erase the need for disposition, monitoring, prevention, or follow-up.
The seventh error is missing counseling and prevention. Students sometimes view counseling as low-yield because it feels less dramatic than resuscitation. In CCS, it is often part of closure. Smoking cessation after COPD or MI, safe sex counseling after STI, diabetic education after hyperglycemia, medication adherence after uncontrolled hypertension, alcohol counseling after pancreatitis, and return precautions after discharge all demonstrate comprehensive care.
The final error is practicing without reviewing why a case went wrong. Repeating cases without feedback can reinforce bad habits. After every practice case, divide missed actions into categories: stabilization, diagnostic testing, treatment, monitoring, location, consult, prevention, or software mechanics. Then practice another case with one specific goal. Deliberate practice works because it narrows attention to correctable behaviors. Passive repetition feels productive, but targeted repetition changes performance.
Train Like CCS Is a Simulation, Not a Reading Assignment
CCS preparation should be active from the beginning.
CCS preparation should be active from the beginning. Reading cases can help build illness scripts, but performance improves when you repeatedly make decisions under simulated conditions. The learning-science rationale is straightforward. Retrieval practice strengthens memory by forcing recall. Simulation with feedback improves procedural fluency by connecting decisions to outcomes. Spaced repetition reduces forgetting. CCS preparation benefits from all three.
Start with a small set of core presentations. Do not begin by chasing rare diagnoses. Master chest pain, dyspnea, abdominal pain, fever, altered mental status, pregnancy complications, endocrine emergencies, neurologic deficits, trauma, pediatric fever, psychiatric emergencies, renal failure, and common outpatient preventive-care scenarios. For each presentation, build a first-minute script. The first-minute script should include setting, safety, urgent diagnostic test, empiric therapy if needed, and what result would change management.
Then run timed cases. During each case, resist the urge to pause and read. Act as you would on exam day. After the case, review carefully. Ask what you missed and classify the miss. Was it a knowledge gap? A sequencing error? A monitoring failure? A software problem? A disposition error? A counseling omission? This classification converts vague frustration into a plan.
A strong review log is more valuable than a stack of completed cases. For example, a log entry might read: “Asthma case: started albuterol and steroids, but forgot repeat pulse oximetry and admission after poor response.” That entry creates a practice target. The next time you see an acute respiratory case, your goal is not “do better.” Your goal is “reassess respiratory status after treatment and decide disposition based on response.” Specificity improves transfer.
| Week | Primary goal | Practice target | Review metric |
|---|---|---|---|
| 1 | Interface fluency | Run common cases untimed, learn order entry and location changes | Can complete core orders without searching |
| 2 | Acute management | Timed cases for shock, chest pain, dyspnea, DKA, stroke, GI bleed | Stabilization orders placed before time advance |
| 3 | Reassessment and disposition | Repeat cases with deliberate monitoring and transfer decisions | Every intervention followed by response check |
| 4 | Exam simulation | Mixed timed blocks, rapid review of missed categories | Fewer repeated omissions across categories |
Use spaced review for missed conditions. If you miss DKA potassium management on Monday, do not only reread it Monday night. Revisit it later in the week, then again after several days. The goal is to make the response automatic when fatigue is high on Day 2. CCS occurs after multiple-choice blocks, so mental efficiency matters. You need scripts that survive fatigue.
Practice should also include “wrong path recovery.” In the real exam, you may order a test that returns unexpectedly or start with a diagnosis that proves wrong. A strong candidate adapts. If a patient with presumed pneumonia worsens and imaging suggests pulmonary embolism, change course. If abdominal pain becomes surgical, escalate. If outpatient therapy fails, admit. CCS rewards updating management as data change.
The MDSteps Platform can support this style when used deliberately. Step 3 learners can pair live vitals CCS cases with an analytics dashboard to identify repeated misses, then use automatic flashcard decks from missed concepts to reinforce scripts between cases. The value is highest when you review patterns, not just completion counts. A completed case is only useful if it changes the next case.
Use Board-Style Clinical Reasoning Inside the Software
CCS cases feel different from multiple-choice questions, but they still use board-style reasoning.
CCS cases feel different from multiple-choice questions, but they still use board-style reasoning. The patient presents with clues. Some clues point to the diagnosis. Others identify severity, contraindications, or the correct setting. The best examinees read the case like a management problem from the first line.
When the patient presents with chest pain, ask whether the pattern is ischemic, pleuritic, tearing, reproducible, exertional, or associated with instability. When the patient presents with abdominal pain, ask about pregnancy, peritonitis, bleeding, obstruction, vascular catastrophe, infection, and surgical disease. When the patient presents with fever, ask whether the patient is septic, immunocompromised, meningitic, postpartum, postoperative, pediatric, or carrying a device. When the patient presents with altered mental status, check glucose early and think about oxygenation, infection, intoxication, metabolic disease, trauma, seizure, and stroke.
These early questions prevent anchoring. Anchoring is dangerous in CCS because a wrong early diagnosis can produce a cascade of wrong orders. The antidote is to identify the life threats before choosing a narrow pathway. A dyspneic patient might have asthma, COPD, heart failure, pulmonary embolism, pneumothorax, pneumonia, anemia, acidosis, anxiety, or foreign body aspiration. You do not need to test everything at once. You do need to notice instability and order the early tests and treatments that distinguish dangerous possibilities.
USMLE logic also favors stepwise management. Stabilize before definitive diagnosis when delay is unsafe. Diagnose before treating when treatment carries meaningful risk and the patient is stable. Treat empirically when the harm of delay exceeds the harm of treatment. Consult when definitive management requires specialty care, but do not abdicate initial management. Admit when monitoring or therapy cannot safely occur outpatient. Discharge when the condition is stable, instructions are clear, and follow-up is appropriate.
Another board-style habit is recognizing distractors. A patient may have a history that tempts you toward a familiar disease, but the vitals tell you the current danger. A patient with anxiety history may still have pulmonary embolism. A young patient may still have ectopic pregnancy. A patient with chronic alcohol use may have pancreatitis, GI bleeding, withdrawal, trauma, infection, or Wernicke encephalopathy. A patient with diabetes may have DKA, hyperosmolar crisis, infection, MI, renal failure, or medication adverse effects. CCS cases may reward broad safety reasoning before narrow diagnosis.
| Cue | What it means | Management implication |
|---|---|---|
| Hypotension, confusion, cool extremities | Possible shock | Higher-acuity setting, IV access, fluids or pressors, urgent cause evaluation |
| Pregnancy potential | Medication and imaging risk | Pregnancy test, pelvic or obstetric pathway when relevant |
| Focal neurologic deficit | Stroke or structural lesion until proven otherwise | Glucose, CT head, time window assessment, stroke pathway |
| Peritoneal signs | Possible surgical abdomen | NPO, IV fluids, analgesia, imaging or surgical consultation |
| Suicidal intent or psychosis | Safety risk | Do not discharge casually, arrange psychiatric evaluation and safety measures |
Clinical reasoning should continue after results return. If the ECG shows STEMI, the case has shifted from chest pain evaluation to reperfusion management. If the pregnancy test is positive in a patient with abdominal pain and hypotension, ectopic pregnancy becomes urgent. If creatinine is high before contrast imaging, adjust the diagnostic plan. If potassium is low in DKA, do not start insulin before correcting it. These pivots show mature management.
Finally, remember that Step 3 is an exam of independent responsibility. It is not only asking whether you can recall facts from Step 1 or choose next best steps from Step 2 CK. It asks whether you can manage a patient through a clinical course. Use the software to demonstrate that you can prioritize, act, reassess, and close the encounter safely.
Rapid-Review Checklist for Exam-Day CCS Performance
The final days before Step 3 should not be spent collecting more scattered facts.
The final days before Step 3 should not be spent collecting more scattered facts. They should be spent tightening execution. A good exam-day CCS plan is short enough to remember and broad enough to apply to every case. The checklist below is designed for that purpose.
Opening move
- Read location, age, chief concern, vitals, and stability first.
- Move unstable patients to the appropriate high-acuity setting.
- Place safety orders before advancing time.
Diagnostic move
- Order the test that changes management fastest.
- Use pregnancy testing when relevant.
- Avoid broad testing in simple stable outpatient cases.
Treatment move
- Treat time-sensitive emergencies before late confirmation.
- Check contraindications before high-risk treatment.
- Control pain, nausea, fever, and respiratory distress appropriately.
Closing move
- Reassess after every major intervention.
- Choose disposition based on stability and monitoring needs.
- Add counseling, prevention, follow-up, and return precautions.
On exam day, do not chase perfection. CCS performance is cumulative. You can still perform well if you miss a minor order, provided the major clinical priorities are correct. The most damaging mistakes are unsafe delays, wrong disposition, missing urgent therapy, failure to monitor response, and harmful unnecessary interventions. Keep returning to the clinical question: what does this patient need now?
Before each case, reset your mind. The previous case is over. Start again with acuity, setting, immediate risks, and a focused plan. If the case seems easy, do not become careless. Easy cases often test completion: discharge instructions, follow-up, preventive counseling, medication safety, or monitoring. If the case seems hard, do not freeze. Stabilize the patient, collect decisive information, treat what cannot wait, and reassess.
Use the final practice block to rehearse your cadence. Read. Stabilize. Order. Advance. Reassess. Adjust. Dispose. Counsel. That rhythm prevents most avoidable omissions. It also keeps you from spending too much time typing low-yield orders. The exam interface rewards organized behavior because organized behavior is safer clinical behavior.
For a last self-audit, review the categories you missed most often in practice. If your misses cluster around monitoring, write a reminder to repeat vitals and response checks. If your misses cluster around disposition, rehearse admission, ICU, operating room, labor and delivery, psychiatric safety, and outpatient follow-up decisions. If your misses cluster around preventive care, rehearse counseling linked to common diagnoses. If your misses cluster around software mechanics, run practice cases until order entry and clock movement feel automatic.
CCS improvement is not mysterious. It comes from aligning your actions with the patient’s risk, practicing the interface, and reviewing errors by category. The better you become at sequencing care, the less the exam feels like a guessing game. You are not trying to impress the software with volume. You are trying to show safe independent management.
To continue practicing, review Step 3 resources at MDSteps Step 3, try clinical reasoning breakdowns at MDSteps sample question breakdowns, and use targeted CCS simulation when your main weakness is timing, reassessment, or disposition.
Daniel R. Alvarez, MD, Internal Medicine.
References
- United States Medical Licensing Examination. Computer-based Case Simulations. https://www.usmle.org/exam-resources/step-3-materials/step-3-test-question-formats/computer-based-case-simulations
- United States Medical Licensing Examination. Step 3 Exam Content. https://www.usmle.org/step-exams/step-3/step-3-exam-content
- United States Medical Licensing Examination. Step 3 Content Outline and Specifications. https://www.usmle.org/exam-resources/step-3-materials/step-3-content-outline-and-specifications
- United States Medical Licensing Examination. Step 3 Sample Test Questions. https://www.usmle.org/prepare-your-exam/step-3-materials/step-3-sample-test-questions
- Federation of State Medical Boards. Step 3. https://www.fsmb.org/step-3/
- Brame CJ, Biel R. Test-enhanced learning: the potential for testing to promote greater learning in undergraduate science courses. CBE Life Sci Educ. 2015;14(2):es4. https://pmc.ncbi.nlm.nih.gov/articles/PMC4477741/
- McGaghie WC, Issenberg SB, Cohen ER, Barsuk JH, Wayne DB. Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review. Acad Med. 2011;86(6):706-711. https://pmc.ncbi.nlm.nih.gov/articles/PMC3102783/
- Trumble E, et al. Systematic review of distributed practice and retrieval practice in health professions education. https://pmc.ncbi.nlm.nih.gov/articles/PMC11078833/
CCS is not just what you order. It is when you order, reassess, and close the case.
MDSteps helps you practice live CCS cases with vitals, orders, labs, time advancement, reassessment, closure, and after-action feedback.
Full access includes Step 1, Step 2 CK, Step 3, CCS cases, analytics, auto-flashcards, and study planning.